Fischer Michael J, Ho P Michael, McDermott Kelly, Lowy Elliott, Parikh Chirag R
BMC Nephrol. 2013 May 20;14:107. doi: 10.1186/1471-2369-14-107.
Chronic kidney disease (CKD) is associated with worse outcomes among patients with acute coronary syndrome (ACS). Less is known about the impact of CKD on longitudinal outcomes among clopidogrel treated patients following ACS.
Using a retrospective cohort design, we identified patients hospitalized with ACS between 10/1/2005 and 1/10/10 at Department of Veterans Affairs (VA) facilities and who were discharged on clopidogrel. Using outpatient serum creatinine values, estimated glomerular filtration rate [eGFR (1.73 ml/min/m2)] was calculated using the CKD-EPI equation. The association between eGFR and mortality, hospitalization for acute myocardial infarction (AMI), and major bleeding were examined using Cox proportional hazards models.
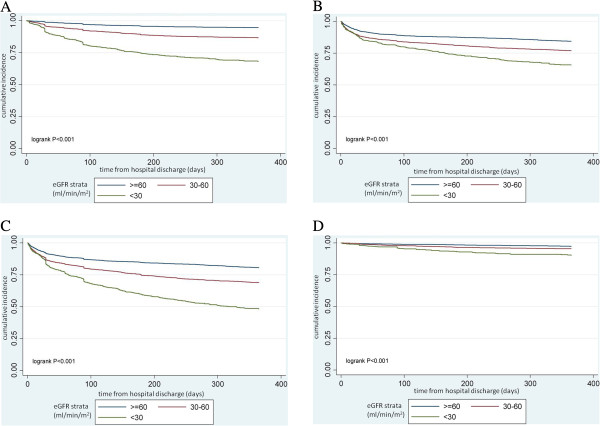
Among 7413 patients hospitalized with ACS and discharged taking clopidogrel, 34.5% had eGFR 30-60 and 11.6% had eGFR < 30. During 1-year follow-up after hospital discharge, 10% of the cohort died, 18% were hospitalized for AMI, and 4% had a major bleeding event. Compared to those with eGFR > =60, individuals with eGFR 30-60 (HR 1.45; 95% CI: 1.18-1.76) and < 30 (HR 2.48; 95% CI: 1.97-3.13) had a significantly higher risk of death. A progressive increased risk of AMI hospitalization was associated with declining eGFR: HR 1.20; 95% CI: 1.04-1.37 for eGFR 30-60 and HR 1.47; 95% CI: 1.22-1.78 for eGFR < 30. eGFR < 30 was independently associated with over a 2-fold increased risk in major bleeding (HR 2.09; 95% CI: 1.40-3.12) compared with eGFR > = 60.
Lower levels of kidney function were associated with higher rates of death, AMI hospitalization, and major bleeding among patients taking clopidogrel after hospitalization for ACS.
慢性肾脏病(CKD)与急性冠脉综合征(ACS)患者的不良预后相关。关于CKD对ACS后接受氯吡格雷治疗患者的长期预后影响的了解较少。
采用回顾性队列设计,我们确定了2005年10月1日至2010年1月10日期间在退伍军人事务部(VA)设施住院并出院时服用氯吡格雷的ACS患者。利用门诊血清肌酐值,采用CKD-EPI方程计算估算肾小球滤过率[eGFR(1.73 ml/min/m²)]。使用Cox比例风险模型检验eGFR与死亡率、急性心肌梗死(AMI)住院率和大出血之间的关联。
在7413例因ACS住院并出院时服用氯吡格雷的患者中,34.5%的患者eGFR为30 - 60,11.6%的患者eGFR<30。出院后1年随访期间,该队列中有10%的患者死亡,18%的患者因AMI住院,4%的患者发生大出血事件。与eGFR≥60的患者相比,eGFR为30 - 60(HR 1.45;95%CI:1.18 - 1.76)和<30(HR 2.48;95%CI:1.97 - 3.13)的患者死亡风险显著更高。AMI住院风险随着eGFR下降而逐渐增加:eGFR为30 - 60时,HR 1.20;95%CI:1.04 - 1.37;eGFR<30时,HR 1.47;95%CI:1.22 - 1.78。与eGFR≥60相比,eGFR<30与大出血风险增加2倍以上独立相关(HR 2.09;95%CI:1.40 - 3.12)。
肾功能水平较低与ACS住院后服用氯吡格雷的患者的较高死亡率、AMI住院率和大出血率相关。