University of California, Los Angeles, Los Angeles, CA 90024, USA.
Ann Intern Med. 2013 May 21;158(10):709-17. doi: 10.7326/0003-4819-158-10-201305210-00005.
Accurate estimation of life expectancy is essential to offering appropriate care to men with early-stage prostate cancer, but mortality risks associated with comorbidity are poorly defined.
To determine the effect of age, comorbidity, and tumor risk on other-cause and prostate cancer-specific mortality in men with early-stage disease.
Prospective cohort study.
A nationally representative, population-based cohort.
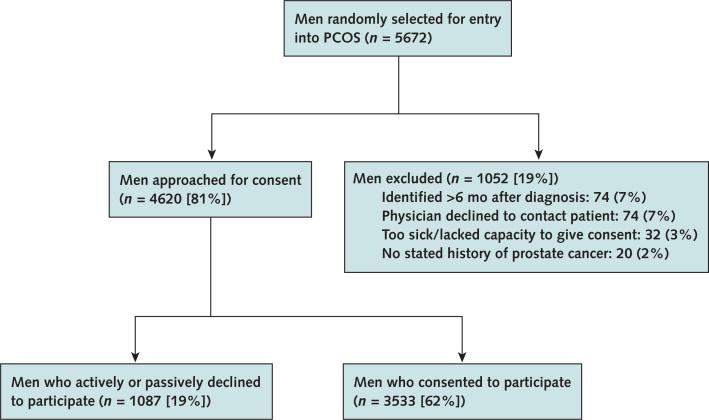
3183 men with nonmetastatic prostate cancer at diagnosis.
Baseline self-reported comorbidity (scored as a count of 12 major comorbid conditions), tumor characteristics, initial treatment, and overall and disease-specific mortality through 14 years of follow-up. Survival analyses that accounted for competing risks were performed.
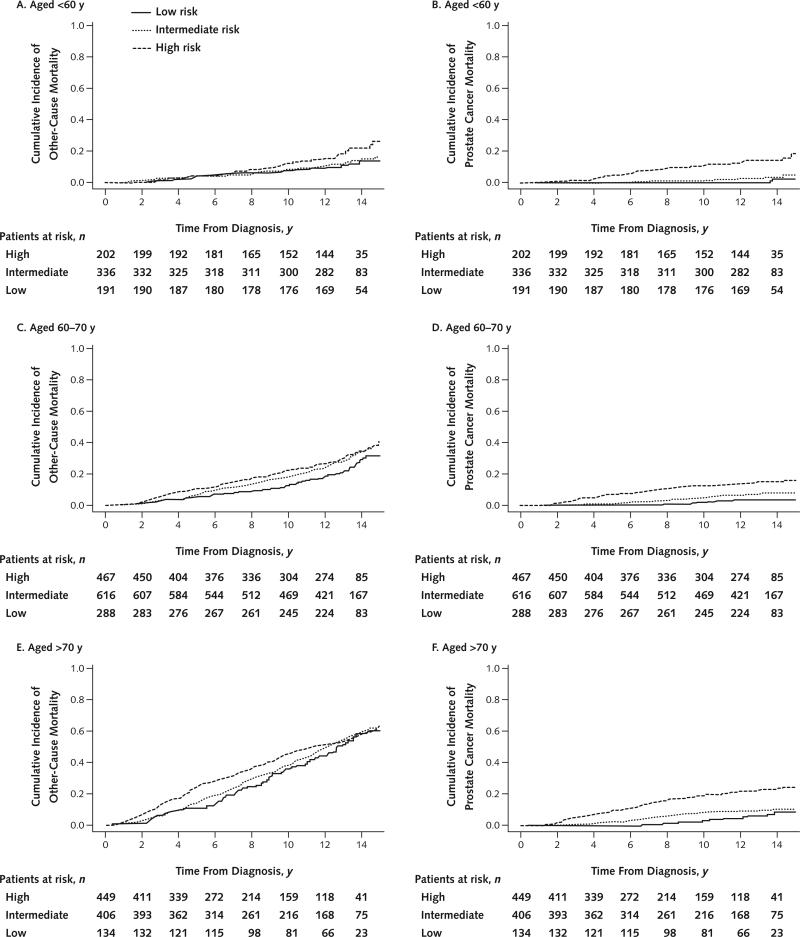
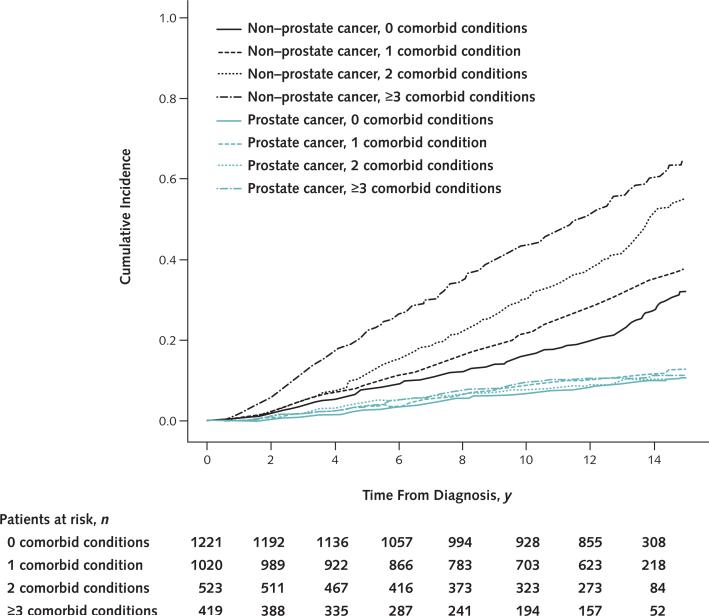
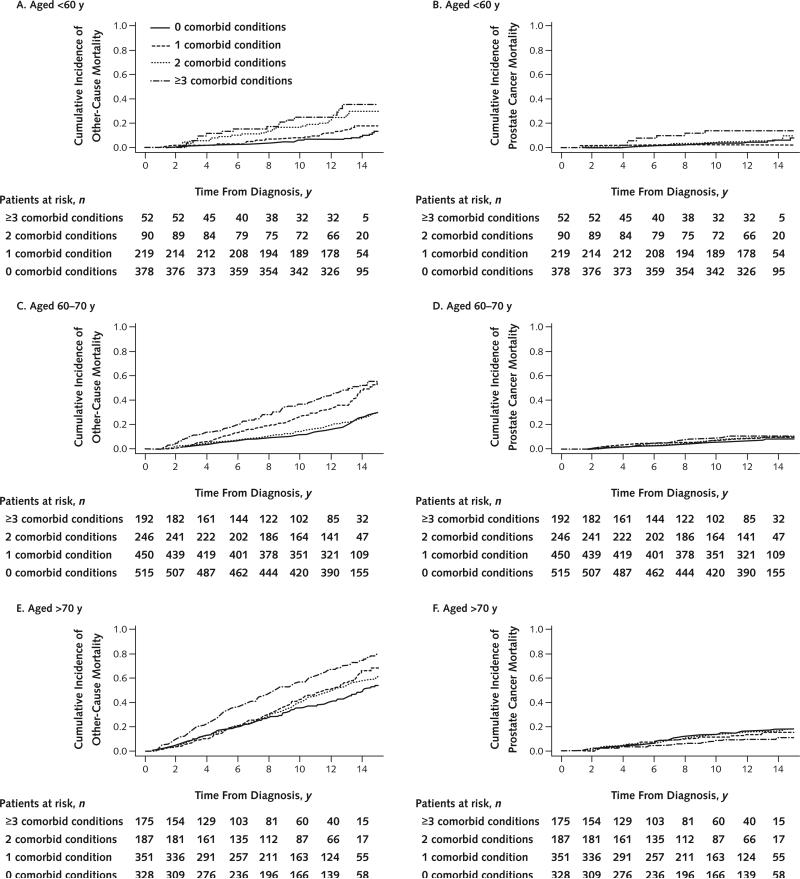
Fourteen-year cumulative other-cause mortality rates were 24%, 33%, 46%, and 57% for men with 0, 1, 2, and 3 or more comorbid conditions, respectively. For men diagnosed at age 65 years, subhazard ratios for other-cause mortality among those with 1, 2, or 3 or more comorbid conditions (vs. none) were 1.2 (95% CI, 1.0 to 1.4), 1.7 (CI, 1.4 to 2.0), and 2.4 (CI, 2.0 to 2.8), respectively. Among men with 3 or more comorbid conditions, 10-year other-cause mortality rates were 26%, 40%, and 71% for those aged 60 years or younger, 61 to 74 years, and 75 years or older at diagnosis, respectively. Prostate cancer-specific mortality was minimal in patients with low-risk (3%) and intermediate-risk (7%) disease but appreciable in those with high-risk disease (18%) and did not vary by number of comorbid conditions (10% to 11% in all groups).
Comorbid conditions were self-reported.
Older men with multiple major comorbid conditions are at high risk for other-cause mortality within 10 years of diagnosis and should consider this information when deciding between conservative management and aggressive treatment for low- or intermediate-risk prostate cancer.
National Cancer Institute.
准确估计预期寿命对于为早期前列腺癌男性提供适当的护理至关重要,但与合并症相关的死亡率定义不明确。
确定年龄、合并症和肿瘤风险对早期疾病男性其他原因和前列腺癌特异性死亡率的影响。
前瞻性队列研究。
全国代表性、基于人群的队列。
3183 名诊断为非转移性前列腺癌的男性。
基线时自我报告的合并症(评分 12 种主要合并症)、肿瘤特征、初始治疗以及 14 年随访期间的总死亡率和疾病特异性死亡率。进行了考虑竞争风险的生存分析。
14 年累积其他原因死亡率分别为 24%、33%、46%和 57%,分别为无合并症、1 种、2 种和 3 种或更多合并症的男性。对于 65 岁诊断的男性,有 1、2 或 3 种或更多合并症(与无合并症相比)的男性其他原因死亡率的亚危险比分别为 1.2(95%CI,1.0 至 1.4)、1.7(CI,1.4 至 2.0)和 2.4(CI,2.0 至 2.8)。在有 3 种或更多合并症的男性中,60 岁或以下、61 至 74 岁和 75 岁或以上诊断的男性 10 年其他原因死亡率分别为 26%、40%和 71%。低危(3%)和中危(7%)疾病患者的前列腺癌特异性死亡率较低,但高危疾病(18%)患者的死亡率较高,且不受合并症数量的影响(所有组的 10%至 11%)。
合并症是自我报告的。
患有多种主要合并症的老年男性在诊断后 10 年内有很高的其他原因死亡率风险,在决定对低危或中危前列腺癌进行保守治疗与积极治疗时,应考虑这一信息。
美国国立癌症研究所。