Department of Pharmacotherapy and Translational Research and Center for Pharmacogenomics, College of Pharmacy, University of Florida, Gainesville, FL, USA.
Hypertension. 2013 Jul;62(1):48-54. doi: 10.1161/HYPERTENSIONAHA.111.00823. Epub 2013 May 20.
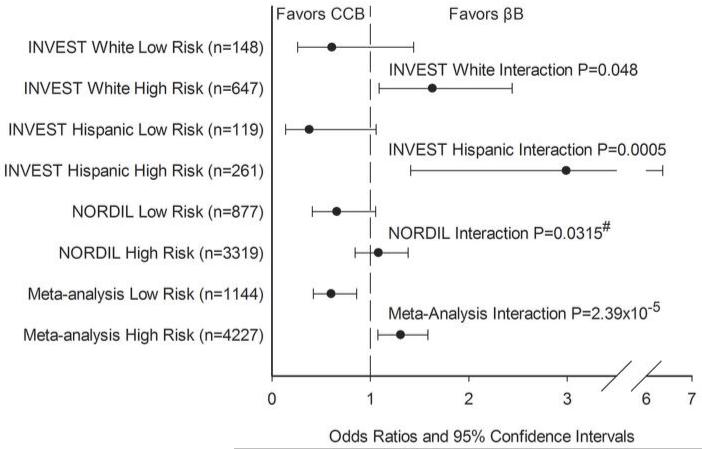
We sought to identify novel pharmacogenetic markers associated with cardiovascular outcomes in patients with hypertension on antihypertensive therapy. We genotyped a 1:4 case:control cohort (n=1345) on the Illumina HumanCVD Beadchip from the INternational VErapamil SR-Trandolapril STudy (INVEST), where participants were randomized to a β-blocker strategy or a calcium channel blocker strategy. Genome-spanning single nucleotide polymorphism (SNP)×treatment interaction analyses of nonsynonymous SNPs were conducted in white and Hispanic race/ethnic groups. Top hits from whites were tested in Hispanics for consistency. A genetic risk score was constructed from the top 3 signals and tested in the Nordic Diltiazem study. SIGLEC12 rs16982743 and A1BG rs893184 had a significant interaction with treatment strategy for adverse cardiovascular outcomes (INVEST whites and Hispanics combined interaction P=0.0038 and 0.0036, respectively). A genetic risk score, including rs16982743, rs893184, and rs4525 in F5, was significantly associated with treatment-related adverse cardiovascular outcomes in whites and Hispanics from the INVEST study and in the Nordic Diltiazem study (meta-analysis interaction P=2.39×10(-5)). In patients with a genetic risk score of 0 or 1, calcium channel blocker treatment was associated with lower risk (odds ratio [95% confidence interval]=0.60 [0.42-0.86]), and in those with a genetic risk score of 2 to 3, calcium channel blocker treatment was associated with higher risk (odds ratio [95% confidence interval]=1.31 [1.08-1.59]). These results suggest that cardiovascular outcomes may differ based on SIGLEC12, A1BG, F5 genotypes, and antihypertensive treatment strategy. These specific genetic associations and our risk score provide insight into a potential approach to personalized antihypertensive treatment selection.
我们试图确定与接受抗高血压治疗的高血压患者心血管结局相关的新型药物遗传学标志物。我们对来自国际维拉帕米 SR-特拉唑嗪研究(INVEST)的 Illumina HumanCVD Beadchip 的 1:4 病例对照队列(n=1345)进行了基因分型,其中参与者被随机分配到β受体阻滞剂策略或钙通道阻滞剂策略。在白人和西班牙裔人群中进行了全基因组单核苷酸多态性(SNP)×治疗相互作用的非 synonymous SNP 分析。在西班牙裔人群中测试了白人的主要发现以确保一致性。从前三个信号构建了遗传风险评分,并在北欧地尔硫卓研究中进行了测试。SIGLEC12 rs16982743 和 A1BG rs893184 与不良心血管结局的治疗策略有显著的相互作用(INVEST 白人和西班牙裔人群合并交互 P=0.0038 和 0.0036)。包括 rs16982743、rs893184 和 F5 中的 rs4525 在内的遗传风险评分与 INVEST 研究和北欧地尔硫卓研究中白人和西班牙裔人群的治疗相关不良心血管结局显著相关(荟萃分析交互 P=2.39×10(-5))。在遗传风险评分为 0 或 1 的患者中,钙通道阻滞剂治疗与较低的风险相关(比值比[95%置信区间]=0.60[0.42-0.86]),而在遗传风险评分为 2 至 3 的患者中,钙通道阻滞剂治疗与较高的风险相关(比值比[95%置信区间]=1.31[1.08-1.59])。这些结果表明,心血管结局可能因 SIGLEC12、A1BG、F5 基因型和抗高血压治疗策略而异。这些特定的遗传关联和我们的风险评分为个性化抗高血压治疗选择提供了新的思路。