Division of Pharmacokinetics and Drug Therapy, Department of Pharmaceutical Biosciences, Uppsala University and Uppsala University Hospital, Uppsala, Sweden.
PLoS One. 2013 May 17;8(5):e62401. doi: 10.1371/journal.pone.0062401. Print 2013.
Appropriateness of prescribing can be assessed by various measures and screening instruments. The aims of this study were to investigate the effects of pharmacists' interventions on appropriateness of prescribing in elderly patients, and to explore the relationship between these results and hospital care utilization during a 12-month follow-up period.
The study population from a previous randomized controlled study, in which the effects of a comprehensive pharmacist intervention on re-hospitalization was investigated, was used. The criteria from the instruments MAI, STOPP and START were applied retrospectively to the 368 study patients (intervention group (I) n = 182, control group (C) n = 186). The assessments were done on admission and at discharge to detect differences over time and between the groups. Hospital care consumption was recorded and the association between scores for appropriateness, and hospitalization was analysed.
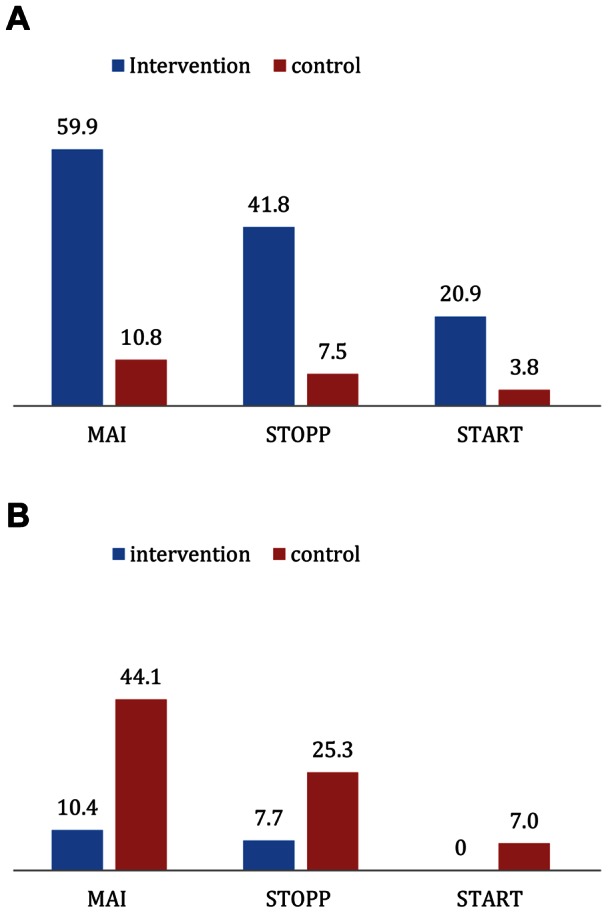
The number of Potentially Inappropriate Medicines (PIMs) per patient as identified by STOPP was reduced for I but not for C (1.42 to 0.93 vs. 1.46 to 1.66 respectively, p<0.01). The number of Potential Prescription Omissions (PPOs) per patient as identified by START was reduced for I but not for C (0.36 to 0.09 vs. 0.42 to 0.45 respectively, p<0.001). The summated score for MAI was reduced for I but not for C (8.5 to 5.0 and 8.7 to 10.0 respectively, p<0.001). There was a positive association between scores for MAI and STOPP and drug-related readmissions (RR 8-9% and 30-34% respectively). No association was detected between the scores of the tools and total re-visits to hospital.
The interventions significantly improved the appropriateness of prescribing for patients in the intervention group as evaluated by the instruments MAI, STOPP and START. High scores in MAI and STOPP were associated with a higher number of drug-related readmissions.
可通过各种措施和筛选工具来评估处方的适宜性。本研究旨在调查药师干预对老年患者处方适宜性的影响,并在 12 个月的随访期间探讨这些结果与医院就诊利用之间的关系。
使用来自先前一项随机对照研究的研究人群,该研究调查了综合药师干预对再住院的影响。回顾性地应用 MAI、STOPP 和 START 工具的标准对 368 名研究患者(干预组 (I) n = 182,对照组 (C) n = 186)进行评估。在入院和出院时进行评估,以检测随时间的差异和组间差异。记录医院就诊消耗,并分析适宜性评分与住院之间的关联。
I 组每位患者的潜在不适当药物(PIMs)数量减少,但 C 组没有(1.42 降至 0.93 比 1.46 升至 1.66,p<0.01)。I 组每位患者的潜在处方遗漏(PPO)数量减少,但 C 组没有(0.36 降至 0.09 比 0.42 升至 0.45,p<0.001)。I 组的 MAI 综合评分降低,但 C 组没有(8.5 降至 5.0 比 8.7 升至 10.0,p<0.001)。MAI 和 STOPP 评分与药物相关再入院之间存在正相关(RR 分别为 8-9%和 30-34%)。工具评分与总就诊次数之间未检测到关联。
干预措施显著改善了干预组患者的处方适宜性,这通过 MAI、STOPP 和 START 工具评估。MAI 和 STOPP 评分高与更多的药物相关再入院相关。