School of Population and Global Health, University of Melbourne, Carlton, Vic 3053, Australia.
BMJ. 2013 May 21;346:f2360. doi: 10.1136/bmj.f2360.
To assess the cancer risk in children and adolescents following exposure to low dose ionising radiation from diagnostic computed tomography (CT) scans.
Population based, cohort, data linkage study in Australia. COHORT MEMBERS: 10.9 million people identified from Australian Medicare records, aged 0-19 years on 1 January 1985 or born between 1 January 1985 and 31 December 2005; all exposures to CT scans funded by Medicare during 1985-2005 were identified for this cohort. Cancers diagnosed in cohort members up to 31 December 2007 were obtained through linkage to national cancer records.
Cancer incidence rates in individuals exposed to a CT scan more than one year before any cancer diagnosis, compared with cancer incidence rates in unexposed individuals.
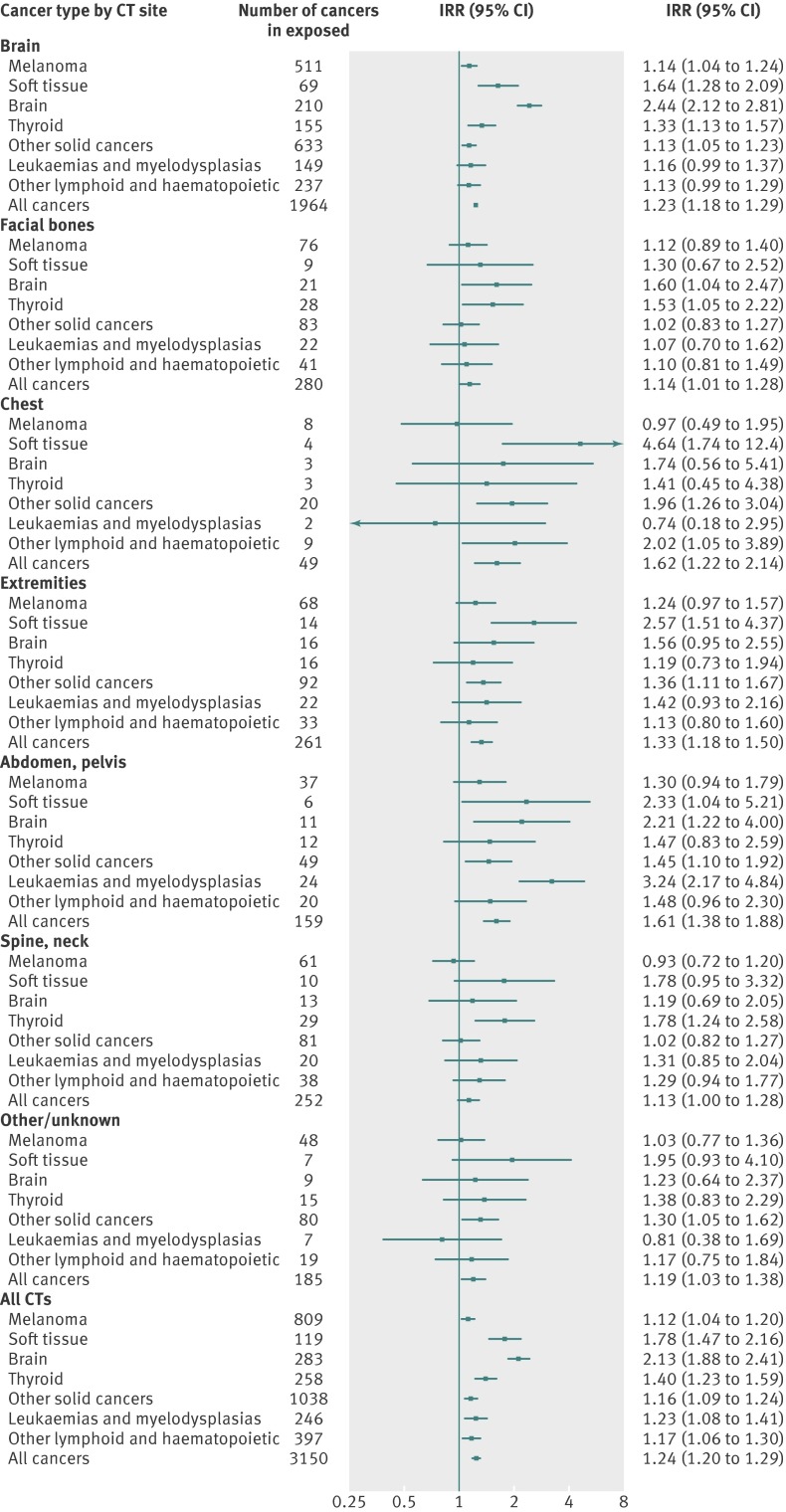
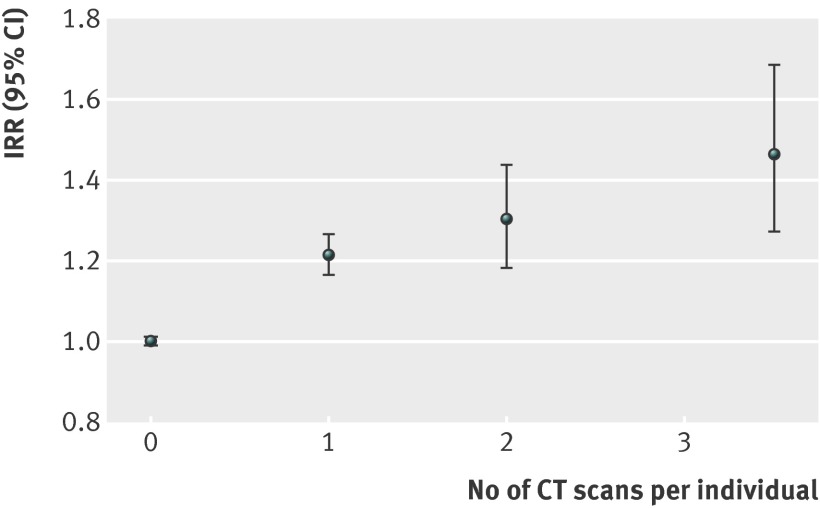
60,674 cancers were recorded, including 3150 in 680,211 people exposed to a CT scan at least one year before any cancer diagnosis. The mean duration of follow-up after exposure was 9.5 years. Overall cancer incidence was 24% greater for exposed than for unexposed people, after accounting for age, sex, and year of birth (incidence rate ratio (IRR) 1.24 (95% confidence interval 1.20 to 1.29); P<0.001). We saw a dose-response relation, and the IRR increased by 0.16 (0.13 to 0.19) for each additional CT scan. The IRR was greater after exposure at younger ages (P<0.001 for trend). At 1-4, 5-9, 10-14, and 15 or more years since first exposure, IRRs were 1.35 (1.25 to 1.45), 1.25 (1.17 to 1.34), 1.14 (1.06 to 1.22), and 1.24 (1.14 to 1.34), respectively. The IRR increased significantly for many types of solid cancer (digestive organs, melanoma, soft tissue, female genital, urinary tract, brain, and thyroid); leukaemia, myelodysplasia, and some other lymphoid cancers. There was an excess of 608 cancers in people exposed to CT scans (147 brain, 356 other solid, 48 leukaemia or myelodysplasia, and 57 other lymphoid). The absolute excess incidence rate for all cancers combined was 9.38 per 100,000 person years at risk, as of 31 December 2007. The average effective radiation dose per scan was estimated as 4.5 mSv.
The increased incidence of cancer after CT scan exposure in this cohort was mostly due to irradiation. Because the cancer excess was still continuing at the end of follow-up, the eventual lifetime risk from CT scans cannot yet be determined. Radiation doses from contemporary CT scans are likely to be lower than those in 1985-2005, but some increase in cancer risk is still likely from current scans. Future CT scans should be limited to situations where there is a definite clinical indication, with every scan optimised to provide a diagnostic CT image at the lowest possible radiation dose.
评估儿童和青少年因接受诊断性计算机断层扫描(CT)扫描而受到低剂量电离辐射的癌症风险。
在澳大利亚进行的基于人群的队列、数据关联研究。
从澳大利亚医疗保险记录中确定的 1090 万人,年龄在 1985 年 1 月 1 日或 1985 年 1 月 1 日之前出生,在 1985 年至 2005 年期间接受 Medicare 资助的所有 CT 扫描均确定为该队列。在 2007 年 12 月 31 日之前,通过与国家癌症记录的链接,确定了队列成员中诊断出的癌症。
与未暴露个体相比,在任何癌症诊断前一年以上接受 CT 扫描的个体的癌症发病率。
共记录了 60674 例癌症,包括 3150 例在 680211 名至少在任何癌症诊断前一年接受 CT 扫描的人。暴露后随访的平均持续时间为 9.5 年。在考虑年龄、性别和出生年份后,暴露人群的总体癌症发病率比未暴露人群高 24%(发病率比(IRR)1.24(95%置信区间 1.20 至 1.29);P<0.001)。我们观察到剂量反应关系,每增加一次 CT 扫描,IRR 增加 0.16(0.13 至 0.19)。在较小年龄暴露时(趋势 P<0.001),IRR 更高。在首次暴露后 1-4 年、5-9 年、10-14 年和 15 年或以上,IRR 分别为 1.35(1.25 至 1.45)、1.25(1.17 至 1.34)、1.14(1.06 至 1.22)和 1.24(1.14 至 1.34)。许多实体癌(消化系统、黑色素瘤、软组织、女性生殖器官、泌尿道、脑和甲状腺);白血病、骨髓增生异常和其他一些淋巴样癌的 IRR 显著增加。在接受 CT 扫描的人群中,有 608 例癌症(147 例脑癌、356 例其他实体癌、48 例白血病或骨髓增生异常、57 例其他淋巴样癌)。截至 2007 年 12 月 31 日,所有癌症合并的绝对超额发病率为每 100000 人年 9.38 例。每次扫描的平均有效辐射剂量估计为 4.5 mSv。
该队列中 CT 扫描暴露后癌症发病率的增加主要归因于辐射。由于在随访结束时癌症仍在继续增加,因此目前尚无法确定 CT 扫描的最终终生风险。目前 CT 扫描的辐射剂量可能低于 1985-2005 年的剂量,但目前的扫描仍可能导致癌症风险增加。未来的 CT 扫描应限于有明确临床指征的情况,每一次扫描都应优化,以尽可能低的辐射剂量提供诊断 CT 图像。