Division of Cardiovascular Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
J Am Heart Assoc. 2013 May 24;2(3):e000174. doi: 10.1161/JAHA.113.000174.
Access site complications contribute to morbidity and mortality during percutaneous coronary intervention (PCI). Transradial arterial access significantly lowers the risk of access site complications compared to transfemoral arteriotomy. We sought to develop a prediction model for access site complications in patients undergoing PCI with femoral arteriotomy, and assess whether transradial access was selectively used in patients at high risk for complications.
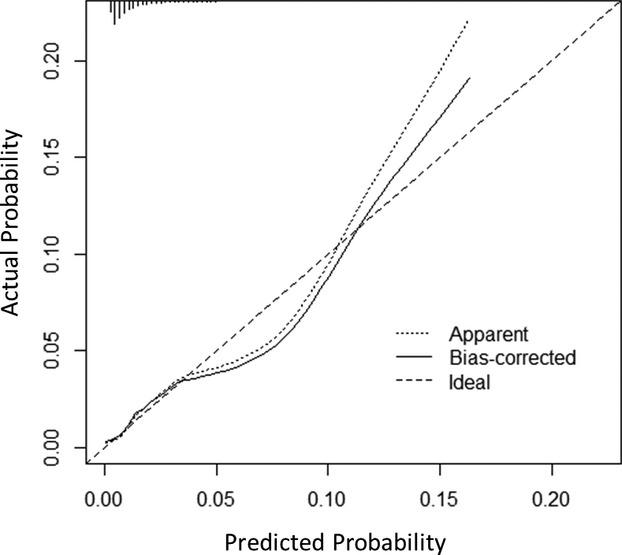
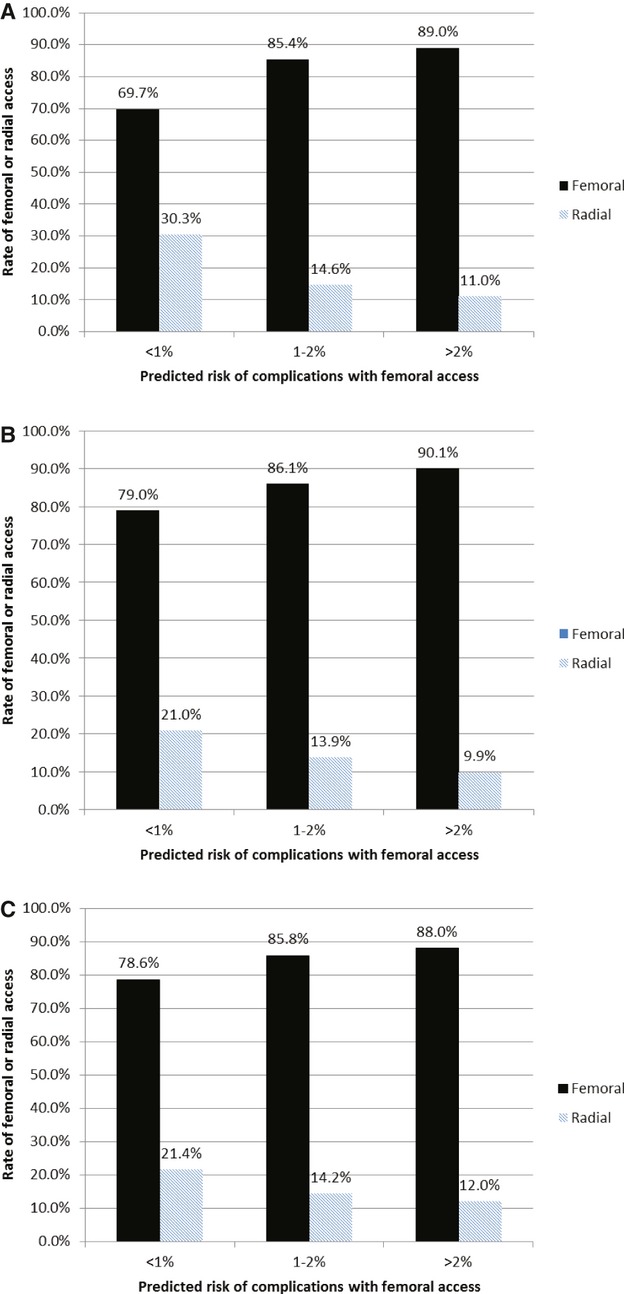
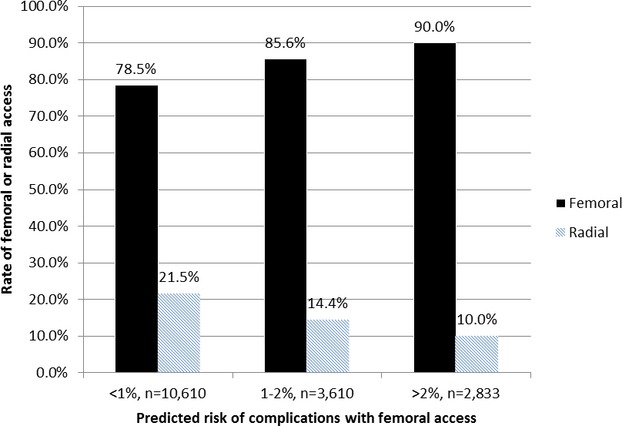
We analyzed 17 509 patients who underwent PCI without circulatory support from 2008 to 2011 at 5 institutions. Transradial arterial access was used in 17.8% of patients. In those who underwent transfemoral access, 177 (1.2%) patients had access site complications. Using preprocedural clinical and demographic data, a prediction model for femoral arteriotomy complications was generated. The variables retained in the model included: elevated age (P<0.001), female gender (P<0.001), elevated troponin (P<0.001), decreased renal function or dialysis (P=0.002), emergent PCI (P=0.01), prior PCI (P=0.005), diabetes (P=0.008), and peripheral artery disease (P=0.003). The model showed moderate discrimination (optimism-adjusted c-statistic=0.72) and was internally validated via bootstrap resampling. Patients with higher predicted risk of complications via transfemoral access were less likely to receive transradial access (P<0.001). Similar results were seen in patients presenting with and without ST-segment myocardial infarction and when adjusting for individual physician operator.
We generated and validated a model for transfemoral access site complications during PCI. Paradoxically, patients most likely to develop access site complications from transfemoral access, and therefore benefit from transradial access, were the least likely to receive transradial access.
经皮冠状动脉介入治疗(PCI)过程中,入路部位并发症可导致发病率和死亡率升高。与经股动脉切开术相比,经桡动脉入路可显著降低入路部位并发症的风险。我们旨在建立一个预测行经股动脉切开术 PCI 患者入路部位并发症的模型,并评估经桡动脉入路是否选择性地应用于并发症风险较高的患者。
我们分析了 2008 年至 2011 年 5 家机构的 17509 例未接受循环支持的 PCI 患者。其中 17.8%的患者采用经桡动脉入路。在接受经股动脉入路的患者中,177 例(1.2%)发生入路部位并发症。使用术前临床和人口统计学数据,建立了经股动脉切开术并发症预测模型。模型中保留的变量包括:高龄(P<0.001)、女性(P<0.001)、肌钙蛋白升高(P<0.001)、肾功能或透析下降(P=0.002)、紧急 PCI(P=0.01)、既往 PCI(P=0.005)、糖尿病(P=0.008)和外周动脉疾病(P=0.003)。该模型具有中等的区分度(经校正后乐观 c 统计量=0.72),通过 bootstrap 重采样进行内部验证。通过经股动脉切开术预测并发症风险较高的患者接受经桡动脉入路的可能性较小(P<0.001)。在有和没有 ST 段抬高心肌梗死的患者中以及在考虑个体术者的情况下,都观察到了类似的结果。
我们建立并验证了一个 PCI 经股动脉入路部位并发症预测模型。矛盾的是,经股动脉切开术入路部位并发症风险最高、因此从经桡动脉入路中获益最大的患者,接受经桡动脉入路的可能性最小。