Department of Surgery, School of Public Health, University of Minnesota, Minneapolis, MN 55455, USA.
JAMA. 2013 Jun 5;309(21):2240-9. doi: 10.1001/jama.2013.5835.
Controlling glycemia, blood pressure, and cholesterol is important for patients with diabetes. How best to achieve this goal is unknown.
To compare Roux-en-Y gastric bypass with lifestyle and intensive medical management to achieve control of comorbid risk factors.
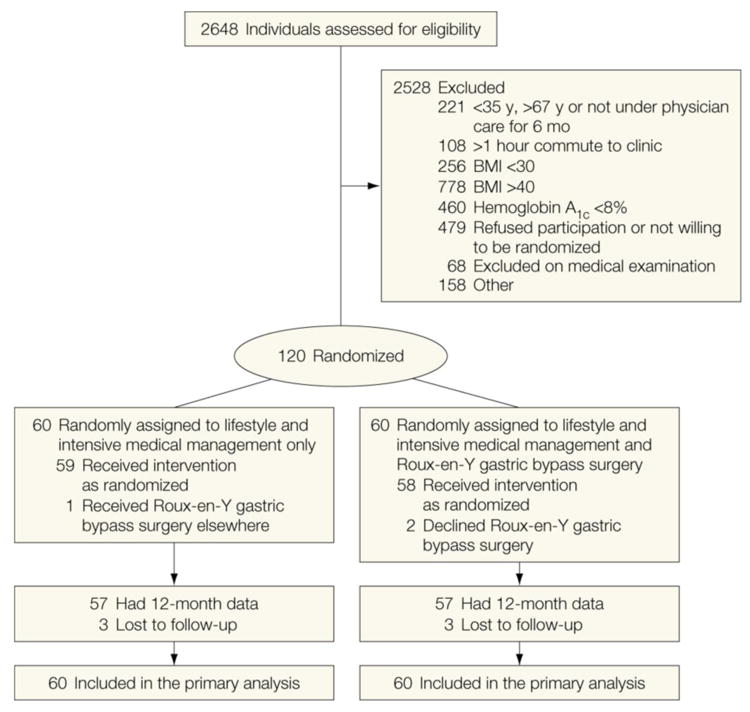
DESIGN, SETTING, AND PARTICIPANTS: A 12-month, 2-group unblinded randomized trial at 4 teaching hospitals in the United States and Taiwan involving 120 participants who had a hemoglobin A1c (HbA1c) level of 8.0% or higher, body mass index (BMI) between 30.0 and 39.9, C peptide level of more than 1.0 ng/mL, and type 2 diabetes for at least 6 months. The study began in April 2008.
Lifestyle-intensive medical management intervention and Roux-en-Y gastric bypass surgery. Medications for hyperglycemia, hypertension, and dyslipidemia were prescribed according to protocol and surgical techniques that were standardized.
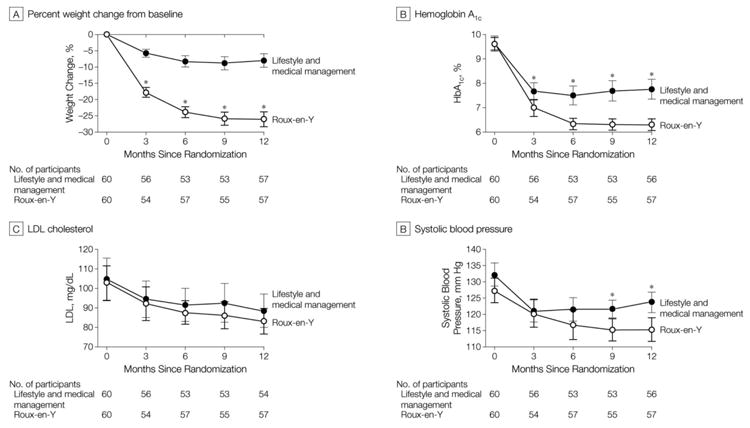
Composite goal of HbA1c less than 7.0%, low-density lipoprotein cholesterol less than 100 mg/dL, and systolic blood pressure less than 130 mm Hg.
All 120 patients received the intensive lifestyle-medical management protocol and 60 were randomly assigned to undergo Roux-en-Y gastric bypass. After 12-months, 28 participants (49%; 95% CI, 36%-63%) in the gastric bypass group and 11 (19%; 95% CI, 10%-32%) in the lifestyle-medical management group achieved the primary end points (odds ratio [OR], 4.8; 95% CI, 1.9-11.7). Participants in the gastric bypass group required 3.0 fewer medications (mean, 1.7 vs 4.8; 95% CI for the difference, 2.3-3.6) and lost 26.1% vs 7.9% of their initial body weigh compared with the lifestyle-medical management group (difference, 17.5%; 95% CI, 14.2%-20.7%). Regression analyses indicated that achieving the composite end point was primarily attributable to weight loss. There were 22 serious adverse events in the gastric bypass group, including 1 cardiovascular event, and 15 in the lifestyle-medical management group. There were 4 perioperative complications and 6 late postoperative complications. The gastric bypass group experienced more nutritional deficiency than the lifestyle-medical management group.
In mild to moderately obese patients with type 2 diabetes, adding gastric bypass surgery to lifestyle and medical management was associated with a greater likelihood of achieving the composite goal. Potential benefits of adding gastric bypass surgery to the best lifestyle and medical management strategies of diabetes must be weighed against the risk of serious adverse events.
clinicaltrials.gov Identifier: NCT00641251.
控制血糖、血压和胆固醇对于糖尿病患者非常重要。但如何最好地实现这一目标尚不清楚。
比较 Roux-en-Y 胃旁路手术与生活方式和强化医学管理,以实现对合并症风险因素的控制。
设计、设置和参与者:在美国和中国台湾的 4 所教学医院进行的一项为期 12 个月、2 组非盲随机试验,共纳入 120 名参与者,他们的糖化血红蛋白(HbA1c)水平为 8.0%或更高,体重指数(BMI)在 30.0 到 39.9 之间,C 肽水平高于 1.0ng/ml,且患有 2 型糖尿病至少 6 个月。研究于 2008 年 4 月开始。
生活方式强化医学管理干预和 Roux-en-Y 胃旁路手术。根据方案和标准化手术技术为高血糖、高血压和血脂异常开具药物。
HbA1c 小于 7.0%、低密度脂蛋白胆固醇小于 100mg/dL 和收缩压小于 130mmHg 的复合目标。
所有 120 名患者均接受强化生活方式医学管理方案治疗,其中 60 名患者被随机分配接受 Roux-en-Y 胃旁路手术。12 个月后,胃旁路组有 28 名参与者(49%;95%置信区间,36%-63%)和生活方式医学管理组有 11 名参与者(19%;95%置信区间,10%-32%)达到主要终点(比值比[OR],4.8;95%置信区间,1.9-11.7)。胃旁路组的参与者需要服用的药物少 3.0 种(平均 1.7 种 vs 4.8 种;95%置信区间差值,2.3-3.6),与生活方式医学管理组相比,体重减轻了 26.1%(初始体重的 7.9%;95%置信区间差值,14.2%-20.7%)。回归分析表明,达到复合终点主要归因于体重减轻。胃旁路组有 22 例严重不良事件,包括 1 例心血管事件,生活方式医学管理组有 15 例。胃旁路组有 4 例围手术期并发症和 6 例术后晚期并发症。胃旁路组比生活方式医学管理组更易出现营养缺乏。
在患有 2 型糖尿病的轻度至中度肥胖患者中,将胃旁路手术与生活方式和医学管理相结合,更有可能达到复合目标。将胃旁路手术加入到 2 型糖尿病的最佳生活方式和医学管理策略中带来的潜在益处,必须与严重不良事件的风险相权衡。
clinicaltrials.gov 标识符:NCT00641251。