Asai Nobuhiro, Kawamura Yasutaka, Yamazaki Ikuo, Sogawa Keiji, Ohkuni Yoshihiro, O'uchi Toshihiro, Kubo Akihito, Yamaguchi Etsuro, Kaneko Norihiro
Department of Pulmonology, Kameda Medical Center, Zip296-8602 929 higashi-cho, kamogawa-city, Chiba, Japan ; Department of Internal Medicine, Division of Respiratory Medicine and Allergology, Aichi Medical University School of Medicine, Aichi, Japan.
Springerplus. 2013 Apr 30;2(1):196. doi: 10.1186/2193-1801-2-196. Print 2013 Dec.
Computed tomography (CT)-guided lung biopsy is commonly used to make a histological diagnosis for pulmonary lesions. Its most common complication is pneumothorax. While it is thought that CT-guided lung biopsy should be avoided in patients with emphysema, however, there is no scientific report documenting the relationship the occurrence of pneumothorax and the severity of emphysema.
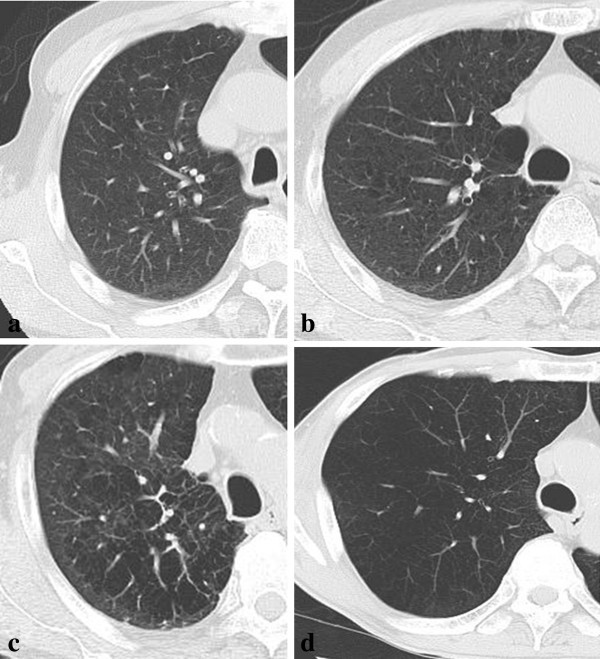
To investigate the relationship between the severity of emphysema and the frequency of pneumothorax, we retrospectively reviewed all the patients who received CT-guided lung biopsy. Severity of emphysema is evaluated by Goddard classification, a visual scale by which areas of vascular disruption and low attenuation value were scored for each lung field of high resolution CT. Patients' characteristics, prognostic accuracy of this method, size and location of the lesion, length of intrapulmonary biopsy paths, and frequency of complications such as pneumothorax or intrapulmonary hemorrhage were evaluated.
One hundred-two patients (69 males and 33 females) received 102 procedures. Diagnostic accuracy was 90.2%. Pneumothorax occurred in 41 of 102 biopsies (40.2%). Chest tube placement was required in 3 out of the 41 cases (7.3%) complicated by pneumothorax (2.9% of all the biopsies). The longer lesion depths from pleura were, the more frequently pneumothorax occurred (6.67 vs 3.66 mm, p=0.019). No correlation was found between location of lesions and frequency of pneumothorax. No significant differences of COPD staging or LAA score were seen between the patients with and without pneumothorax (5.73 vs 4.32 points, p=0.339).
We suggest that severity of emphysema such as stage I or II COPD may not be related to the frequency of pneumothorax.
计算机断层扫描(CT)引导下的肺活检常用于对肺部病变进行组织学诊断。其最常见的并发症是气胸。虽然人们认为肺气肿患者应避免进行CT引导下的肺活检,然而,尚无科学报告记录气胸的发生与肺气肿严重程度之间的关系。
为了研究肺气肿严重程度与气胸发生率之间的关系,我们回顾性分析了所有接受CT引导下肺活检的患者。肺气肿的严重程度通过戈达德分类法进行评估,这是一种视觉评分系统,通过高分辨率CT对每个肺野的血管破坏区域和低衰减值进行评分。评估了患者的特征、该方法的预后准确性、病变的大小和位置、肺内活检路径的长度以及气胸或肺内出血等并发症的发生率。
102例患者(69例男性和33例女性)接受了102次手术。诊断准确率为90.2%。102例活检中有41例(40.2%)发生气胸。41例气胸并发症患者中有3例(7.3%)需要放置胸管(占所有活检的2.9%)。距胸膜的病变深度越长,气胸发生越频繁(6.67对3.66毫米,p = 0.019)。未发现病变位置与气胸发生率之间存在相关性。气胸患者与非气胸患者之间的慢性阻塞性肺疾病(COPD)分期或肺实质面积(LAA)评分无显著差异(5.73对4.32分,p = 0.339)。
我们认为,如I期或II期COPD等肺气肿的严重程度可能与气胸发生率无关。