Royal Children's Hospital, Parkville VIC 3052, Australia.
BMJ. 2013 Jun 10;346:f3092. doi: 10.1136/bmj.f3092.
To determine whether general practice surveillance for childhood obesity, followed by obesity management across primary and tertiary care settings using a shared care model, improves body mass index and related outcomes in obese children aged 3-10 years.
Randomised controlled trial.
22 family practices (35 participating general practitioners) and a tertiary weight management service (three paediatricians, two dietitians) in Melbourne, Australia.
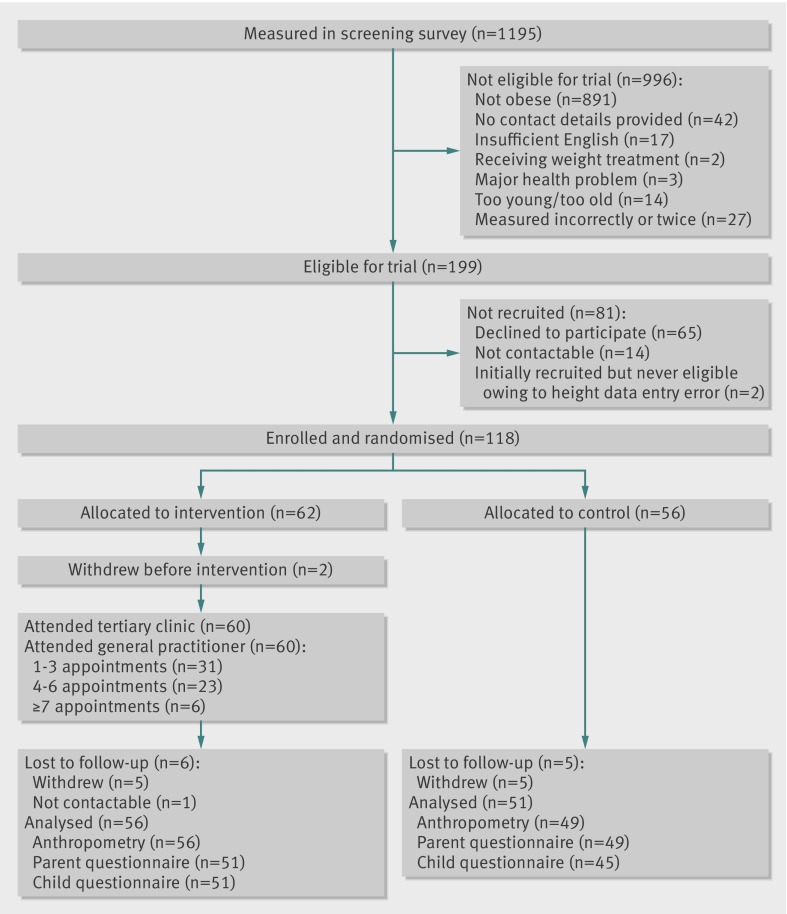
Children aged 3-10 years with body mass index above the 95th centile recruited through their general practice between July 2009 and April 2010.
Children were randomly allocated to one tertiary appointment followed by up to 11 general practice consultations over one year, supported by shared care, web based software (intervention) or "usual care" (control). Researchers collecting outcome measurements, but not participants, were blinded to group assignment.
Children's body mass index z score (primary outcome), body fat percentage, waist circumference, physical activity, quality of diet, health related quality of life, self esteem, and body dissatisfaction and parents' body mass index (all 15 months post-enrolment).
118 (60 intervention, 56 control) children were recruited and 107 (91%) were retained and analysed (56 intervention, 51 control). All retained intervention children attended the tertiary appointment and their general practitioner for at least one (mean 3.5 (SD 2.5, range 1-11)) weight management consultation. At outcome, children in the two trial arms had similar body mass index (adjusted mean difference -0.1 (95% confidence interval -0.7 to 0.5; P=0.7)) and body mass index z score (-0.05 (-0.14 to 0.03); P=0.2). Similarly, no evidence was found of benefit or harm on any secondary outcome. Outcomes varied widely in the combined cohort (mean change in body mass index z score -0.20 (SD 0.25, range -0.97-0.47); 26% of children resolved from obese to overweight and 2% to normal weight.
Although feasible, not harmful, and highly rated by both families and general practitioners, the shared care model of primary and tertiary care management did not lead to better body mass index or other outcomes for the intervention group compared with the control group. Improvements in body mass index in both groups highlight the value of untreated controls when determining efficacy.
Australian New Zealand Clinical Trials Registry ACTRN12608000055303.
确定在初级和三级保健环境中使用共享护理模式对肥胖儿童进行一般实践监测,随后进行肥胖管理,是否可以改善 3-10 岁肥胖儿童的体重指数和相关结果。
随机对照试验。
澳大利亚墨尔本的 22 个家庭实践(35 名参与的全科医生)和一个三级体重管理服务(三名儿科医生,两名营养师)。
2009 年 7 月至 2010 年 4 月期间通过其一般实践招募的年龄在 3-10 岁、体重指数超过第 95 百分位数的儿童。
儿童被随机分配到一个三级预约,然后在一年的时间内进行多达 11 次的一般实践咨询,由共享护理、基于网络的软件(干预组)或“常规护理”(对照组)支持。收集结果测量的研究人员,但不是参与者,对组分配保持盲态。
儿童的体重指数 z 分数(主要结果)、体脂百分比、腰围、身体活动、饮食质量、健康相关生活质量、自尊和身体不满以及父母的体重指数(所有结果均在入组后 15 个月测量)。
招募了 118 名(60 名干预组,56 名对照组)儿童,其中 107 名(91%)保留并进行了分析(56 名干预组,51 名对照组)。所有保留的干预组儿童均至少参加了一次三级预约和他们的全科医生的一次(平均 3.5(SD 2.5,范围 1-11))体重管理咨询。在结局时,两组的体重指数相似(调整后的平均差异-0.1(95%置信区间-0.7 至 0.5;P=0.7))和体重指数 z 分数(-0.05(-0.14 至 0.03);P=0.2)。同样,在联合队列中也没有发现任何益处或危害的证据。在两组中,体重指数 z 分数的变化范围很广(平均变化-0.20(SD 0.25,范围-0.97-0.47));26%的儿童从肥胖转为超重,2%转为正常体重。
尽管初级和三级保健管理的共享护理模式是可行的、无伤害的,并且得到了家庭和全科医生的高度评价,但与对照组相比,该模式并没有导致干预组的体重指数或其他结果更好。两组体重指数的改善突出了在确定疗效时未治疗对照组的价值。
澳大利亚新西兰临床试验注册 ACTRN12608000055303。