Kathirvel Murugesan, Subramanian Shanmuga, Clivio Alessandro, Arun Gandhi, Fogliata Antonella, Nicolini Giorgia, Subramani Vellaiyan, Swamy Shanmugam Thirumalai, Vanetti Eugenio, Cozzi Luca
Radiat Oncol. 2013 Jun 11;8:140. doi: 10.1186/1748-717X-8-140.
The accuracy of the two dose calculation engines available for RapidArc planning (both released for clinical use) is investigated in comparison to the COMPASS data.
Two dose calculation algorithms (Acuros-XB and Anisotropic Analytic Algorithm (AAA)) were used to calculate RA plans and compared to calculations with the Collapsed Cone Convolution algorithm (CC) from the COMPASS system (IBA Dosimetry). CC calculations, performed on patient data, are based on experimental fluence measurements with a 2D array of ion chambers mounted on the linac head. The study was conducted on clinical cases treated with RA. Five cases for each of the following groups were included: Brain, Head and Neck, Thorax, Pelvis and stereotactic body radiation therapy for hypo-fractionated treatments with small fields. COMPASS measurements were performed with the iMatrixx-2D array. RapidArc plans were optimized for delivery using 6MV photons from a Clinac-iX (Varian, Palo Alto, USA).
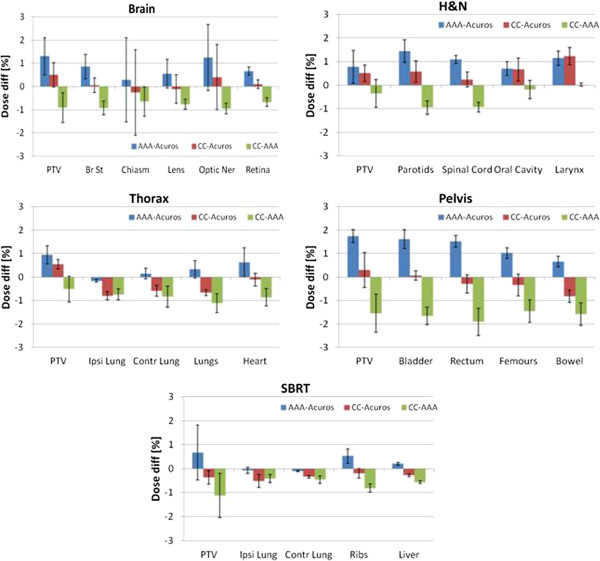
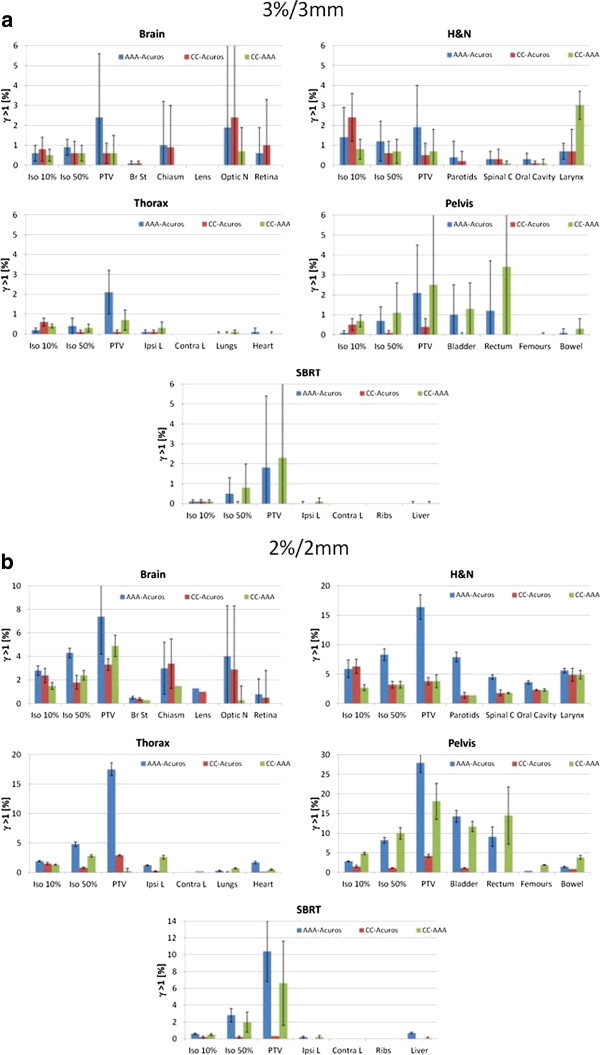
For almost all parameters, the better agreement was between Acuros-XB and COMPASS independently from the anatomical site and fractionation. The same result was obtained from the mean dose difference per organ with Acuros-CC average differences below 0.5% while for AAA-CC data, average deviations exceeded 0.5% and in the case of the pelvis 1%. Relevance of observed differences determined with the 3D gamma analysis resulted in a pass rate exceeding 99.5% for Acuros-CC and exceeding 97.5% for AAA-CC.
This study demonstrated that i) a good agreement exists between COMPASS-CC calculations based on measured fluences with respect to dose distributions obtained with both Acuros-XB and AAA algorithms; ii) 3D dose distributions reconstructed from actual delivery coincide very precisely with the planned data; iii) a slight preference in favor of Acuros-XB was observed suggesting the preference for this algorithm in clinical applications.
将用于容积旋转调强放疗(RapidArc)计划的两种剂量计算引擎(均已发布用于临床)的准确性与COMPASS数据进行比较研究。
使用两种剂量计算算法(Acuros-XB和各向异性解析算法(AAA))来计算容积旋转调强放疗计划,并与COMPASS系统(IBA剂量学)的坍缩圆锥卷积算法(CC)计算结果进行比较。对患者数据进行的CC计算基于使用安装在直线加速器头部的二维电离室阵列进行的实验注量测量。该研究针对接受容积旋转调强放疗治疗的临床病例展开。纳入了以下每组各5个病例:脑、头颈部、胸部、骨盆以及小野低分割立体定向体部放射治疗。使用iMatrixx-2D阵列进行COMPASS测量。容积旋转调强放疗计划使用来自Clinac-iX(美国帕洛阿尔托瓦里安公司)的6MV光子进行优化以用于治疗。
对于几乎所有参数,无论解剖部位和分割方式如何,Acuros-XB与COMPASS之间的一致性更好。从每个器官的平均剂量差异也得到相同结果,Acuros-CC平均差异低于0.5%,而对于AAA-CC数据,平均偏差超过0.5%,在骨盆病例中为1%。通过三维伽马分析确定的观察差异的相关性导致Acuros-CC的通过率超过99.5%,AAA-CC的通过率超过97.5%。
本研究表明:i)基于测量注量的COMPASS-CC计算与使用Acuros-XB和AAA算法获得的剂量分布之间存在良好的一致性;ii)从实际治疗重建的三维剂量分布与计划数据非常精确地吻合;iii)观察到略微倾向于Acuros-XB,表明在临床应用中更倾向于使用该算法。