Unit of Airway Inflammation and Immunology, Department of Experimental Medical Sciences, Lund University, Lund, Sweden.
Respir Res. 2013 Jun 11;14(1):65. doi: 10.1186/1465-9921-14-65.
De novo lymphatic vessel formation has recently been observed in lungs of patients with moderate chronic obstructive pulmonary disease (COPD). However, the distribution of lymphatic vessel changes among the anatomical compartments of diseased lungs is unknown. Furthermore, information regarding the nature of lymphatic vessel alterations across different stages of COPD is missing. This study performs a detailed morphometric characterization of lymphatic vessels in major peripheral lung compartments of patients with different severities of COPD and investigates the lymphatic expression of molecules involved in immune cell trafficking.
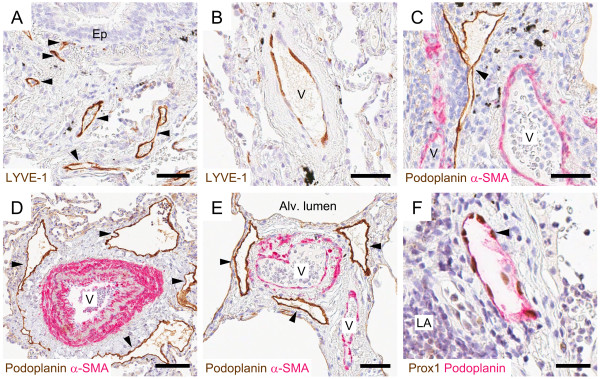
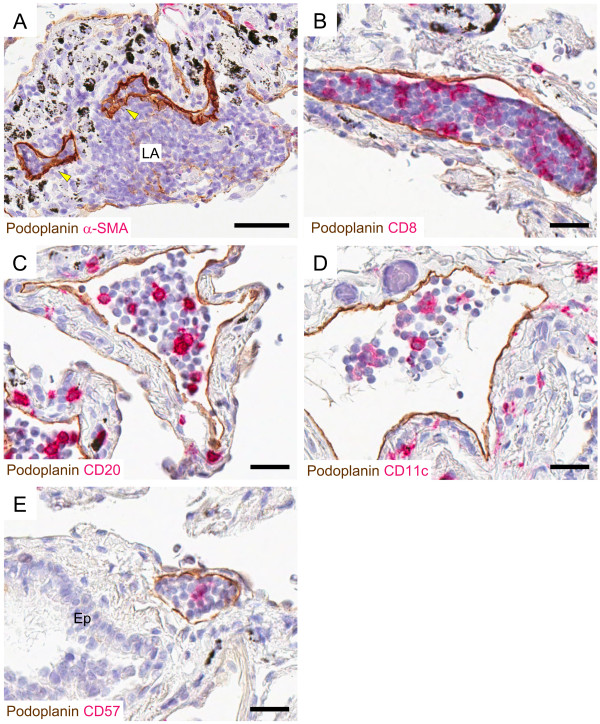
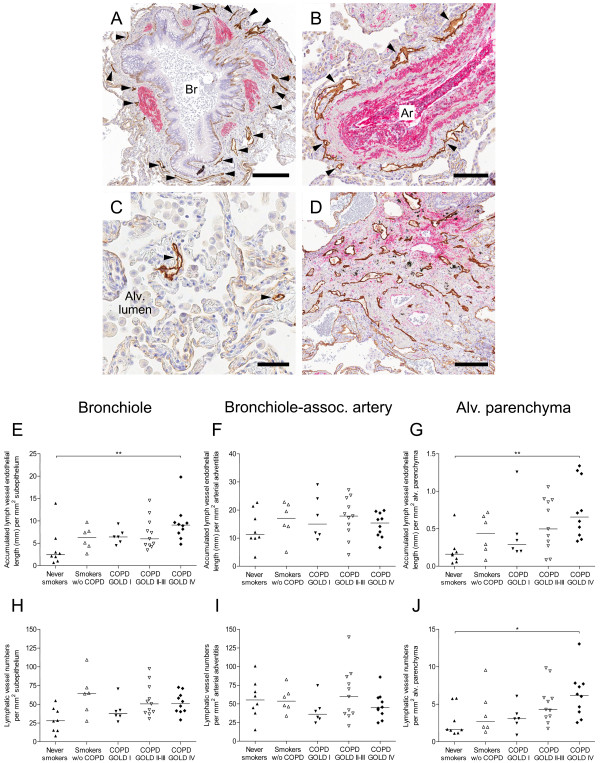
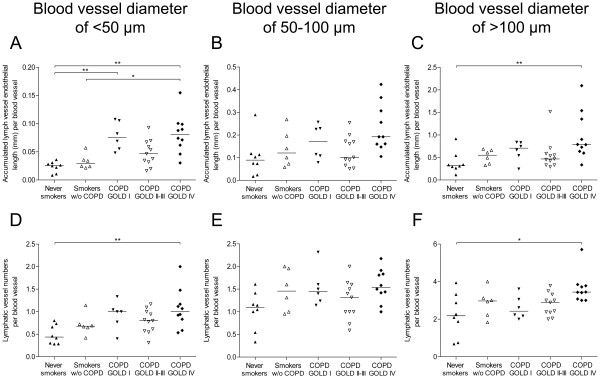
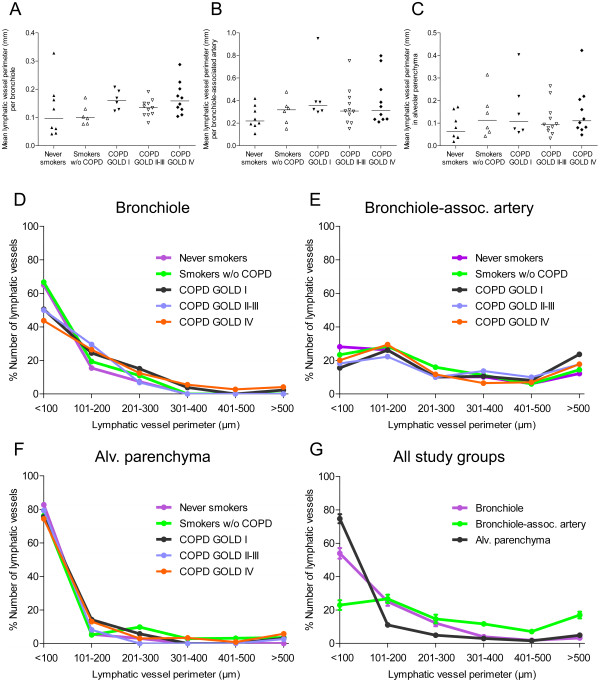
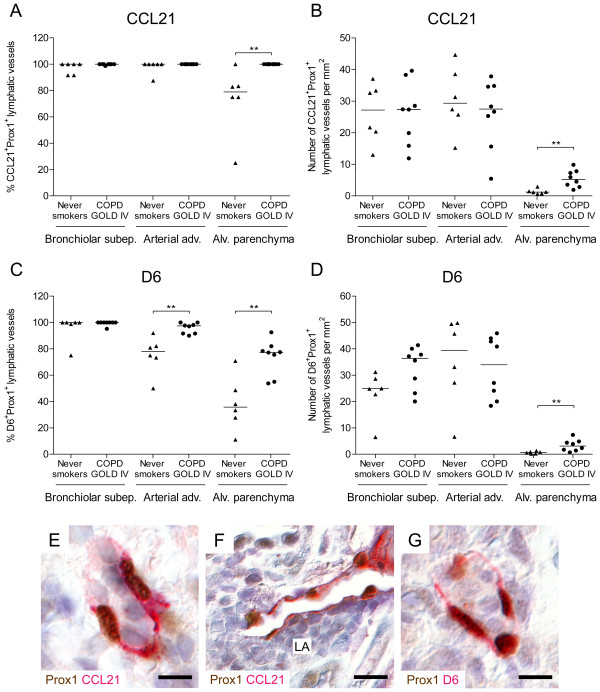
Peripheral lung resection samples obtained from patients with mild (GOLD stage I), moderate-severe (GOLD stage II-III), and very severe (GOLD stage IV) COPD were investigated for podoplanin-immunopositive lymphatic vessels in distinct peripheral lung compartments: bronchioles, pulmonary blood vessels and alveolar walls. Control subjects with normal lung function were divided into never smokers and smokers. Lymphatics were analysed by multiple morphological parameters, as well as for their expression of CCL21 and the chemokine scavenger receptor D6.
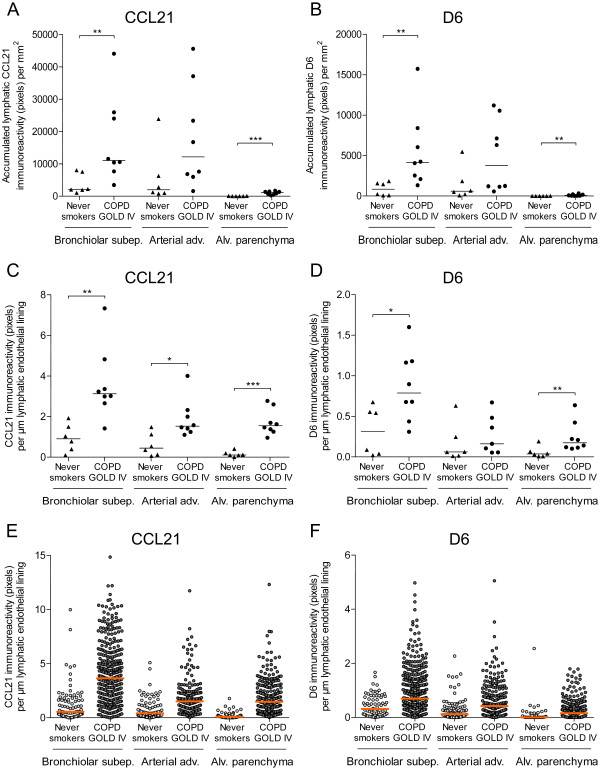
The number of lymphatics increased by 133% in the alveolar parenchyma in patients with advanced COPD compared with never-smoking controls (p < 0.05). In patchy fibrotic lesions the number of alveolar lymphatics increased 20-fold from non-fibrotic parenchyma in the same COPD patients. The absolute number of lymphatics per bronchiole and artery was increased in advanced COPD, but numbers were not different after normalization to tissue area. Increased numbers of CCL21- and D6-positive lymphatics were observed in the alveolar parenchyma in advanced COPD compared with controls (p < 0.01). Lymphatic vessels also displayed increased mean levels of immunoreactivity for CCL21 in the wall of bronchioles (p < 0.01) and bronchiole-associated arteries (p < 0.05), as well as the alveolar parenchyma (p < 0.001) in patients with advanced COPD compared with never-smoking controls. A similar increase in lymphatic D6 immunoreactivity was observed in bronchioles (p < 0.05) and alveolar parenchyma (p < 0.01).
This study shows that severe stages of COPD is associated with increased numbers of alveolar lymphatic vessels and a change in lymphatic vessel phenotype in major peripheral lung compartments. This novel histopathological feature is suggested to have important implications for distal lung immune cell traffic in advanced COPD.
最近在患有中度慢性阻塞性肺疾病(COPD)的患者的肺部观察到新的淋巴管形成。然而,病变肺部解剖部位的淋巴管变化分布尚不清楚。此外,关于 COPD 不同阶段淋巴管改变的信息也缺失。本研究对不同严重程度 COPD 患者的主要外周肺隔室中的淋巴管进行详细的形态计量学描述,并研究参与免疫细胞迁移的分子的淋巴管表达。
研究了轻度(GOLD 分期 I)、中度-重度(GOLD 分期 II-III)和非常严重(GOLD 分期 IV)COPD 患者的外周肺切除样本中的足突蛋白免疫阳性淋巴管,分别位于不同的外周肺隔室:细支气管、肺血管和肺泡壁。正常肺功能的对照组分为从不吸烟者和吸烟者。通过多个形态参数以及趋化因子 CCL21 和趋化因子清除受体 D6 的表达来分析淋巴管。
与从不吸烟者相比,晚期 COPD 患者的肺泡实质中淋巴管数量增加了 133%(p<0.05)。在局灶性纤维化病变中,同一 COPD 患者的非纤维化实质中肺泡淋巴管数量增加了 20 倍。晚期 COPD 患者的每根细支气管和动脉的淋巴管数量增加,但归一化到组织面积后,数量没有差异。与对照组相比,晚期 COPD 患者的肺泡实质中 CCL21 和 D6 阳性淋巴管数量增加(p<0.01)。与从不吸烟者相比,COPD 患者的细支气管壁(p<0.01)和细支气管相关动脉(p<0.05)以及肺泡实质(p<0.001)中淋巴管的 CCL21 免疫反应平均水平也升高。在细支气管(p<0.05)和肺泡实质(p<0.01)中观察到类似的 D6 淋巴管免疫反应增加。
本研究表明,严重的 COPD 与肺泡淋巴管数量增加以及主要外周肺隔室中淋巴管表型改变有关。这种新的组织病理学特征提示在晚期 COPD 中远端肺免疫细胞迁移具有重要意义。