Department of Pharmacy, Brigham and Women's Hospital, Boston, MA, USA.
Ther Clin Risk Manag. 2013;9:277-84. doi: 10.2147/TCRM.S45412. Epub 2013 Jun 5.
Early clinical trials of recombinant human activated protein C (rhAPC) for severe sepsis excluded patients at high risk of bleeding. Recent literature suggests bleeding rates are higher in clinical practice and may be associated with worsened outcomes. Our objective was to evaluate baseline demographics; incidence, and risk factors for major bleeding; and mortality of patients receiving rhAPC for severe sepsis at our institution.
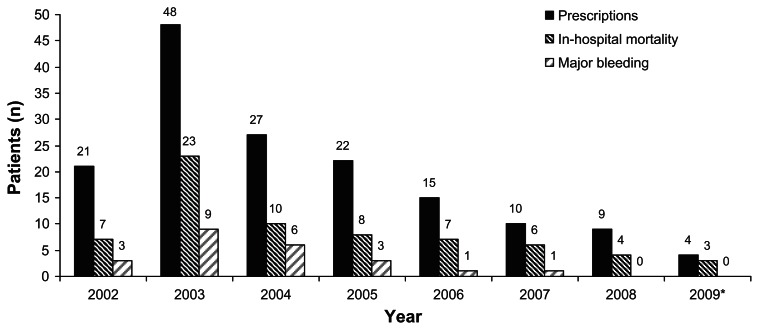
A retrospective study was performed for all patients receiving rhAPC for treatment of severe sepsis at a tertiary academic medical center from January 2002 to June 2009. Demographic information, clinical variables, intensive care unit, and hospital outcomes were recorded.
Of the 156 patients that received rhAPC, 54 (34.6%) did not meet institutional criteria for safe use at baseline due to bleeding precaution or contraindication. Twenty-three (14.7%) patients experienced a major bleeding event. Multivariate analysis demonstrated baseline International Normalized Ratio ≥2.5 (odds ratio [OR] 3.68, 95% confidence interval [CI]: 1.28-10.56; P = 0.03) and platelet count ≤100 × 10(3)/mm(3) (OR 2.86, 95% CI: 1.07-7.67; P = 0.01) as significant predictors of a major bleed. Overall hospital mortality was 57.7%. Multivariate analysis demonstrated the presence of ≥3 organ dysfunctions (OR 2.46, 95% CI: 1.19-5.09; P < 0.05) and medical intensive care unit admission (OR 1.99, 95% CI: 1.00-3.98; P = 0.05) were independent variables associated with hospital mortality.
Patients receiving rhAPC at our institution had higher APACHE II scores, mortality, and major bleeding events than published postmarketing studies. Risk factors for major bleeding other than package-labeling contraindications and bleeding precautions were identified in our patient population.
重组人活化蛋白 C(rhAPC)治疗严重脓毒症的早期临床试验排除了出血风险较高的患者。最近的文献表明,临床实践中的出血率较高,并且可能与预后恶化有关。我们的目的是评估本机构接受 rhAPC 治疗严重脓毒症的患者的基线人口统计学特征、主要出血的发生率和危险因素,以及死亡率。
对 2002 年 1 月至 2009 年 6 月期间在一家三级学术医疗中心接受 rhAPC 治疗严重脓毒症的所有患者进行了回顾性研究。记录了人口统计学信息、临床变量、重症监护病房和医院转归。
在接受 rhAPC 治疗的 156 例患者中,有 54 例(34.6%)由于出血预防或禁忌症,在基线时不符合机构安全使用标准。23 例(14.7%)患者发生了主要出血事件。多变量分析显示,基线国际标准化比值≥2.5(比值比[OR]3.68,95%置信区间[CI]:1.28-10.56;P=0.03)和血小板计数≤100×10³/mm³(OR 2.86,95%CI:1.07-7.67;P=0.01)是主要出血的显著预测因素。总的医院死亡率为 57.7%。多变量分析显示,存在≥3 个器官功能障碍(OR 2.46,95%CI:1.19-5.09;P<0.05)和入住内科重症监护病房(OR 1.99,95%CI:1.00-3.98;P=0.05)是与医院死亡率相关的独立变量。
与上市后研究相比,本机构接受 rhAPC 治疗的患者的 APACHE II 评分、死亡率和主要出血事件更高。在我们的患者人群中,除了包装标签禁忌症和出血预防措施外,还确定了其他主要出血的危险因素。