Welch Center for Prevention, Epidemiology and Clinical Research, Johns Hopkins University, Baltimore, MD; Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
Am J Kidney Dis. 2013 Oct;62(4):691-702. doi: 10.1053/j.ajkd.2013.04.010. Epub 2013 Jun 13.
Estimated glomerular filtration rate (eGFR) and albuminuria are central for diagnosis, staging, and risk evaluation in chronic kidney disease (CKD). Universal thresholds regardless of age, sex, and race are recommended, but relatively little is known about how these demographic factors alter the relationship of eGFR and albuminuria to cardiovascular outcomes.
Observational cohort study.
SETTING & PARTICIPANTS: 11,060 whites and blacks aged 52-75 years in the Atherosclerosis Risk in Communities (ARIC) Study with median follow-up of 11.2 years.
eGFR by the CKD-EPI (CKD Epidemiology Collaboration) creatinine equation (reference, 95 mL/min/1.73 m(2)) and urinary albumin-creatinine ratio (ACR; reference, 5 mg/g).
Cardiovascular events (coronary disease, stroke, and heart failure) and all-cause mortality.
Adjusted HRs associated with eGFR and ACR in subgroups according to age, sex, and race.
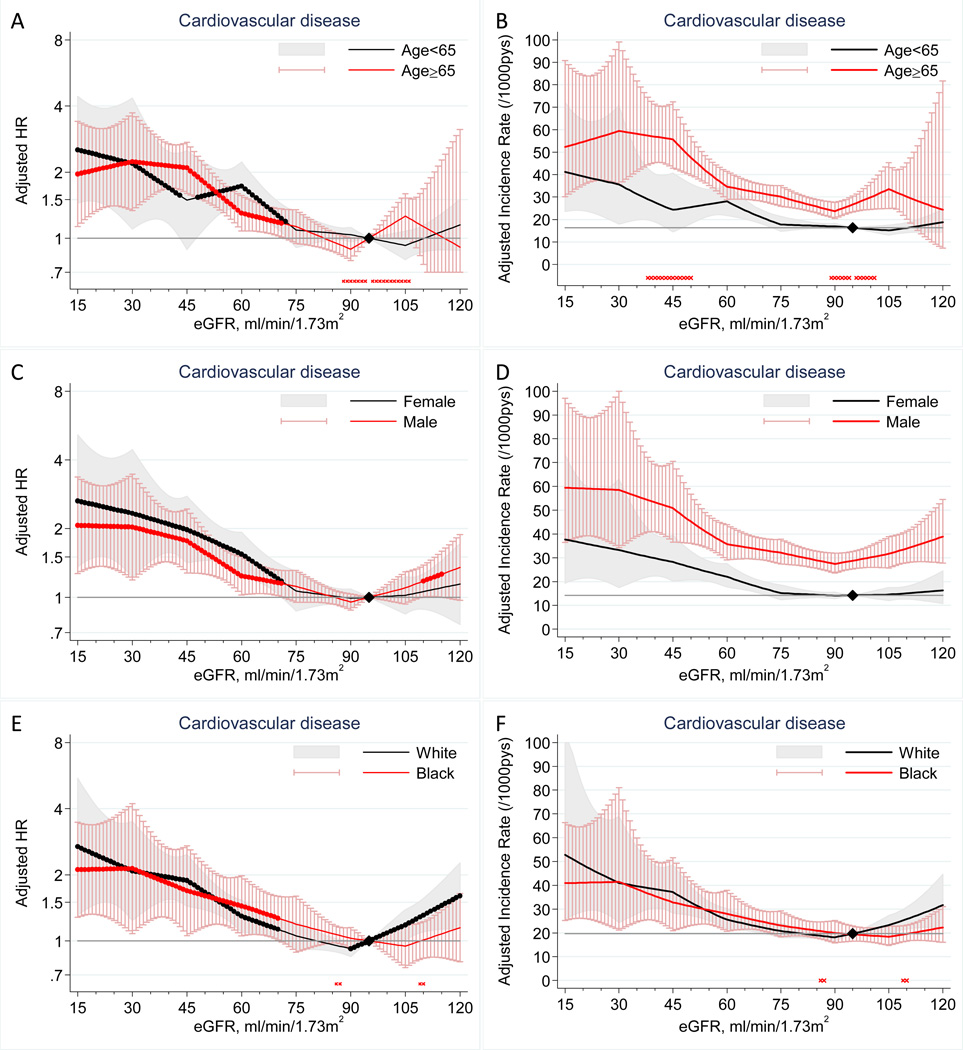
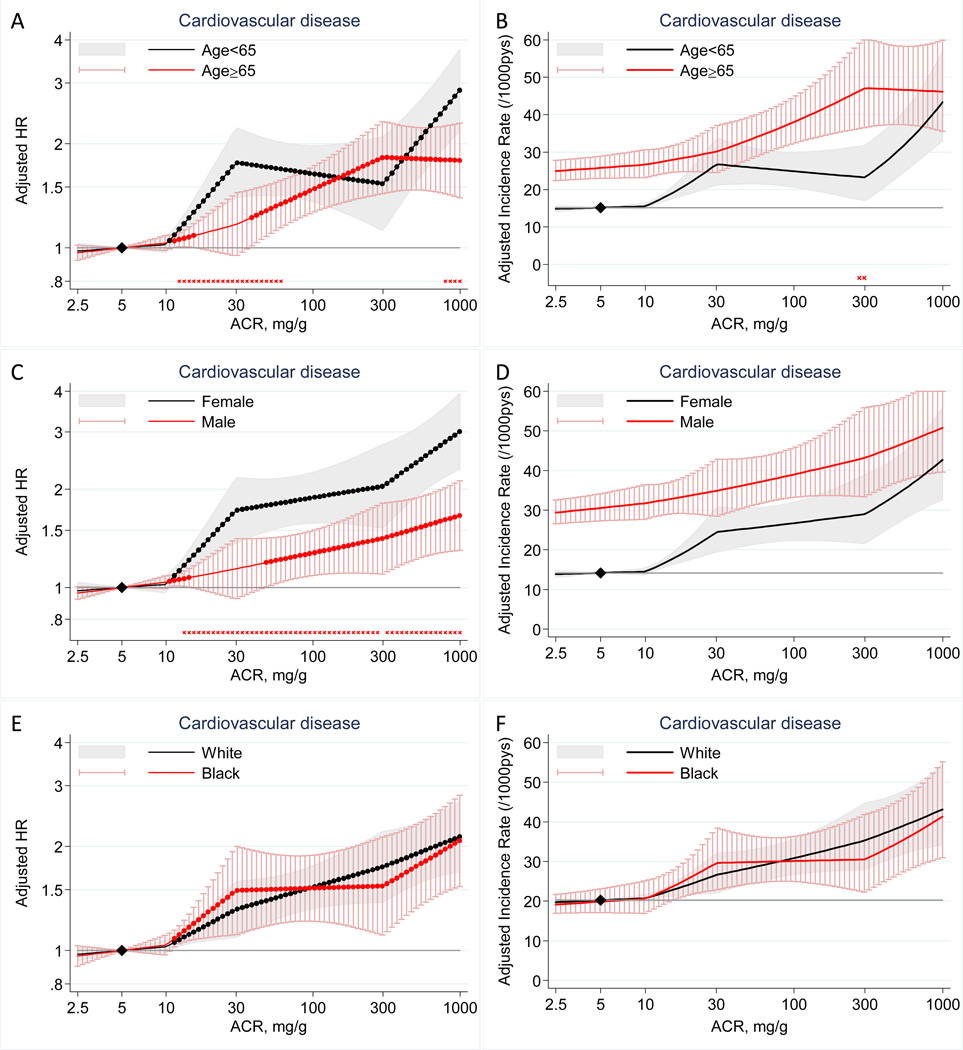
Cardiovascular risk significantly increased at eGFR <70 mL/min/1.73 m(2) in all subgroups according to age (<65 vs ≥65 years), sex, and race (P for interaction >0.2 for these subgroups; eg, at eGFR of 30 mL/min/1.73 m(2), the adjusted HR was 2.19 [95% CI, 1.10-4.35] at age 52-64 years vs 2.23 [95% CI, 1.33-3.72] at age 65-75 years). Results were similar for mortality. Log(ACR) was associated linearly with cardiovascular risk without threshold effects in all subgroups, with some quantitative interactions. HRs according to ACR tended to be lower in men versus women (eg, at ACR of 40 mg/g, 1.18 [95% CI, 0.98-1.41] vs 1.77 [95% CI, 1.45-2.15]) and in the older versus younger population (1.24 [95% CI, 1.04-1.49] vs 1.73 [95% CI, 1.42-2.12]; P for interaction <0.01 for sex and age). Less evident interactions were observed for mortality.
Single measurement of eGFR with creatinine and ACR and relatively narrow age range.
The associations of eGFR and ACR with cardiovascular events were largely similar, with some quantitative interactions, in age, sex, and racial subgroups, generally supporting universal thresholds of GFR and ACR for CKD definition/staging.
估算肾小球滤过率(eGFR)和白蛋白尿是慢性肾脏病(CKD)诊断、分期和风险评估的核心。建议使用不分年龄、性别和种族的通用阈值,但关于这些人口统计学因素如何改变 eGFR 和白蛋白尿与心血管结局的关系,我们知之甚少。
观察性队列研究。
年龄在 52-75 岁的 11060 名白人和黑人参加了动脉粥样硬化风险社区(ARIC)研究,中位随访时间为 11.2 年。
使用 CKD-EPI(CKD 流行病学合作)肌酐方程(参考值,95mL/min/1.73m²)和尿白蛋白/肌酐比值(ACR;参考值,5mg/g)计算 eGFR。
心血管事件(冠心病、中风和心力衰竭)和全因死亡率。
根据年龄、性别和种族,在亚组中与 eGFR 和 ACR 相关的调整后 HR。
根据年龄(<65 岁与≥65 岁)、性别和种族,所有亚组中 eGFR<70mL/min/1.73m²时心血管风险显著增加(P 值交互作用>0.2;例如,在 eGFR 为 30mL/min/1.73m²时,年龄在 52-64 岁的调整 HR 为 2.19[95%CI,1.10-4.35],而年龄在 65-75 岁的调整 HR 为 2.23[95%CI,1.33-3.72])。死亡率的结果也相似。所有亚组中,log(ACR)与心血管风险呈线性相关,无阈值效应,存在一定的定量交互作用。与女性相比,男性的 ACR 相关 HR 往往较低(例如,在 ACR 为 40mg/g 时,1.18[95%CI,0.98-1.41] vs. 1.77[95%CI,1.45-2.15]),在较年轻的人群中也较低(例如,在 ACR 为 40mg/g 时,1.18[95%CI,0.98-1.41] vs. 1.77[95%CI,1.45-2.15])。年龄交互作用<0.01)。与死亡率相比,观察到的交互作用不太明显。
仅测量一次 eGFR 与肌酐和 ACR,年龄范围较窄。
eGFR 和 ACR 与心血管事件的相关性在年龄、性别和种族亚组中基本相似,存在一定的定量交互作用,这通常支持通用的 GFR 和 ACR 阈值用于 CKD 的定义/分期。