Allegretti Andrew S, Steele David J R, David-Kasdan Jo Ann, Bajwa Ednan, Niles John L, Bhan Ishir
Crit Care. 2013 Jun 20;17(3):R109. doi: 10.1186/cc12780.
Continuous renal replacement therapy (CRRT) is a widely used but resource-intensive treatment. Despite its broad adoption in intensive care units (ICUs), it remains challenging to identify patients who would be most likely to achieve positive outcomes with this therapy and to provide realistic prognostic information to patients and families.
We analyzed a prospective cohort of all 863 ICU patients initiated on CRRT at an academic medical center from 2008 to 2011 with either new-onset acute kidney injury (AKI) or pre-admission end-stage renal disease (ESRD). We examined in-hospital and post-discharge mortality (for all patients), as well as renal recovery (for AKI patients). We identified prognostic factors for both in-hospital and post-discharge mortality separately in patients with AKI or ESRD.
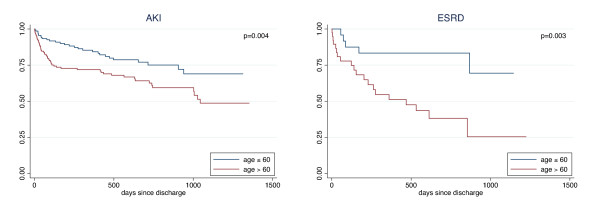
In-hospital mortality was 61% for AKI and 54% for ESRD. In patients with AKI (n=725), independent risk factors for mortality included age over 60 (OR 1.9, 95% CI 1.3, 2.7), serum lactate over 4 mmol/L (OR 2.2, 95% CI 1.5, 3.1), serum creatinine over 3 mg/dL at time of CRRT initiation (OR 0.63, 95% CI 0.43, 0.92) and comorbid liver disease (OR 1.75, 95% CI 1.1, 2.9). Among patients with ESRD (n=138), liver disease was associated with increased mortality (OR 3.4, 95% CI 1.1, 11.1) as was admission to a medical (vs surgical) ICU (OR 2.2, 95% CI 1.1, 4.7). Following discharge, advanced age became a predictor of mortality in both groups (AKI: HR 1.9, 95% CI 1.2, 3.0; ESRD: HR 4.1, 95% CI 1.5, 10.9). At the end of the study period, only 25% (n=183) of patients with AKI achieved dialysis-free survival.
Among patients initiating CRRT, risk factors for mortality differ between patients with underlying ESRD or newly acquired AKI. Long-term dialysis-free survival in AKI is low. Providers should consider these factors when assessing prognosis or appropriateness of CRRT.
连续性肾脏替代疗法(CRRT)是一种广泛应用但资源密集型的治疗方法。尽管它在重症监护病房(ICU)中被广泛采用,但识别最有可能通过这种疗法获得积极结果的患者,并向患者及其家属提供现实的预后信息仍然具有挑战性。
我们分析了2008年至2011年在一家学术医疗中心开始接受CRRT治疗的所有863例ICU患者的前瞻性队列,这些患者患有新发急性肾损伤(AKI)或入院前终末期肾病(ESRD)。我们检查了住院期间和出院后的死亡率(所有患者),以及肾脏恢复情况(AKI患者)。我们分别确定了AKI或ESRD患者住院期间和出院后死亡率的预后因素。
AKI患者的住院死亡率为61%,ESRD患者为54%。在AKI患者(n=725)中,死亡的独立危险因素包括年龄超过60岁(OR 1.9,95%CI 1.3,2.7)、血清乳酸超过4 mmol/L(OR 2.2,95%CI 1.5,3.1)、CRRT开始时血清肌酐超过3 mg/dL(OR 0.63,95%CI 0.43,0.92)和合并肝病(OR 1.75,95%CI 1.1,2.9)。在ESRD患者(n=138)中,肝病与死亡率增加相关(OR 3.4,95%CI 1.1,11.1),入住内科(相对于外科)ICU也与死亡率增加相关(OR 2.2,95%CI 1.1,4.7)。出院后,高龄成为两组患者死亡的预测因素(AKI:HR 1.9,95%CI 1.2,3.0;ESRD:HR 4.1,95%CI 1.5,10.9)。在研究期结束时,只有25%(n=183)的AKI患者实现了无透析生存。
在开始接受CRRT治疗的患者中,潜在ESRD患者和新发生AKI患者的死亡危险因素不同。AKI患者长期无透析生存的比例较低。医疗服务提供者在评估CRRT的预后或适用性时应考虑这些因素。