Robinson Bruce M, Zhang Jinyao, Morgenstern Hal, Bradbury Brian D, Ng Leslie J, McCullough Keith P, Gillespie Brenda W, Hakim Raymond, Rayner Hugh, Fort Joan, Akizawa Tadao, Tentori Francesca, Pisoni Ronald L
1] Arbor Research Collaborative for Health, Ann Arbor, Michigan, USA [2] Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, USA.
Arbor Research Collaborative for Health, Ann Arbor, Michigan, USA.
Kidney Int. 2014 Jan;85(1):158-65. doi: 10.1038/ki.2013.252. Epub 2013 Jun 26.
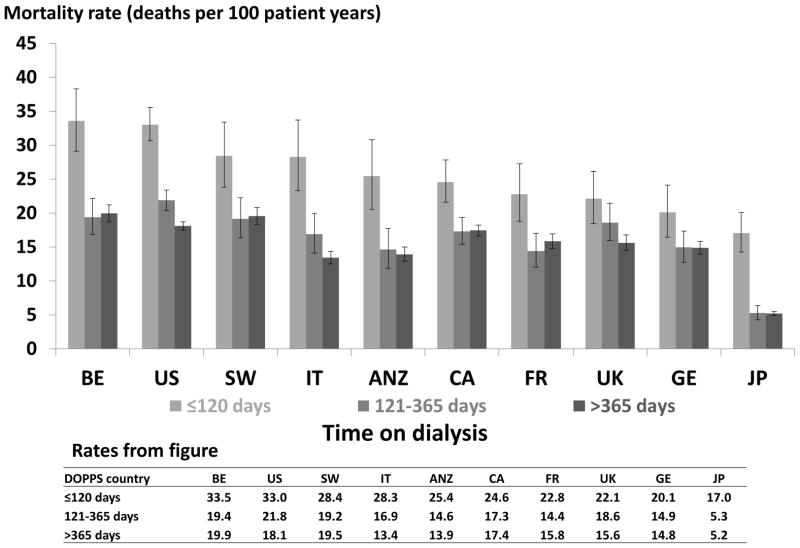
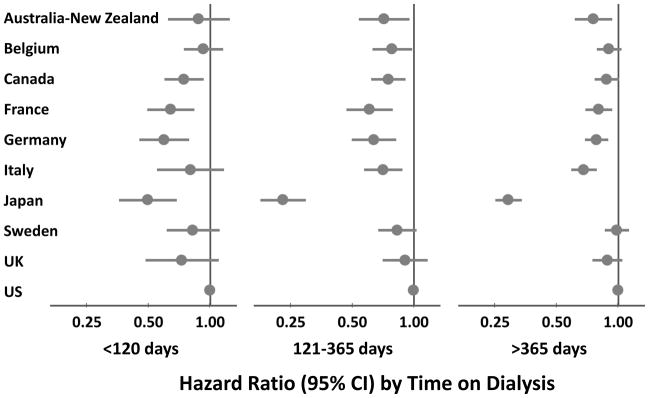
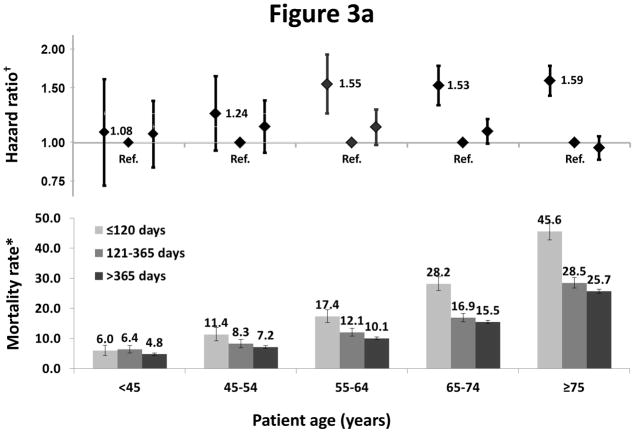
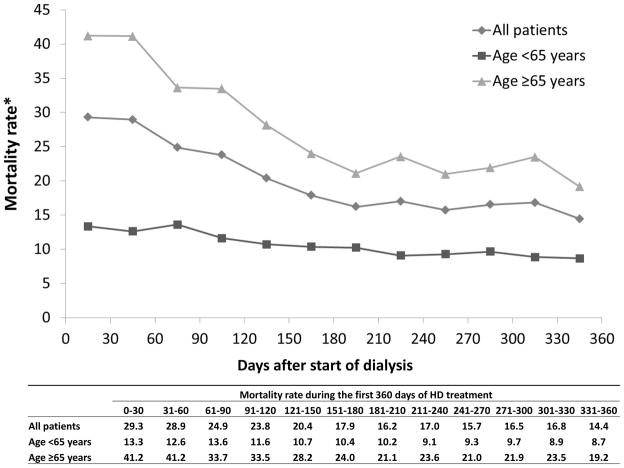
Mortality rates for maintenance hemodialysis patients are much higher than the general population and are even greater soon after starting dialysis. Here we analyzed mortality patterns in 86,886 patients in 11 countries focusing on the early dialysis period using data from the Dialysis Outcomes and Practice Patterns Study, a prospective cohort study of in-center hemodialysis. The primary outcome was all-cause mortality, using time-dependent Cox regression, stratified by study phase adjusted for age, sex, race, and diabetes. The main predictor was time since dialysis start as divided into early (up to 120 days), intermediate (121-365 days), and late (over 365 days) periods. Mortality rates (deaths/100 patient-years) were 26.7 (95% confidence intervals 25.6-27.9), 16.9 (16.2-17.6), and 13.7 (13.5-14.0) in the early, intermediate, and late periods, respectively. In each country, mortality was higher in the early compared to the intermediate period, with a range of adjusted mortality ratios from 3.10 (2.22-4.32) in Japan to 1.15 (0.87-1.53) in the United Kingdom. Adjusted mortality rates were similar for intermediate and late periods. The ratio of elevated mortality rates in the early to the intermediate period increased with age. Within each period, mortality was higher in the United States than in most other countries. Thus, internationally, the early hemodialysis period is a high-risk time for all countries studied, with substantial differences in mortality between countries. Efforts to improve outcomes should focus on the transition period and the first few months of dialysis.
维持性血液透析患者的死亡率远高于普通人群,且在开始透析后不久死亡率更高。在此,我们利用透析结果与实践模式研究(一项针对中心血液透析的前瞻性队列研究)的数据,分析了11个国家86886例患者在透析早期的死亡模式。主要结局为全因死亡率,采用时间依赖性Cox回归分析,按研究阶段分层,并对年龄、性别、种族和糖尿病进行校正。主要预测因素为透析开始后的时间,分为早期(至多120天)、中期(121 - 365天)和晚期(超过365天)。早期、中期和晚期的死亡率(每100患者年的死亡数)分别为26.7(95%置信区间25.6 - 27.9)、16.9(16.2 - 17.6)和13.7(13.5 - 14.0)。在每个国家,早期死亡率均高于中期,校正后的死亡率比值范围从日本的3.10(2.22 - 4.32)到英国的1.15(0.87 - 1.53)。中期和晚期的校正死亡率相似。早期与中期死亡率升高的比值随年龄增加。在每个时间段内,美国的死亡率高于大多数其他国家。因此,在国际上,透析早期对所有研究国家而言都是高风险时期,各国之间的死亡率存在显著差异。改善预后的努力应聚焦于过渡期和透析的头几个月。