Vascular Medicine and Metabolism Unit, University Hospital Sant Joan, IISPV, CIBERDEM, Rovira and Virgili University, Sant Llorenç, 21. 43201-Reus, Spain.
Cardiovasc Diabetol. 2013;12 Suppl 1(Suppl 1):S2. doi: 10.1186/1475-2840-12-S1-S2. Epub 2013 May 30.
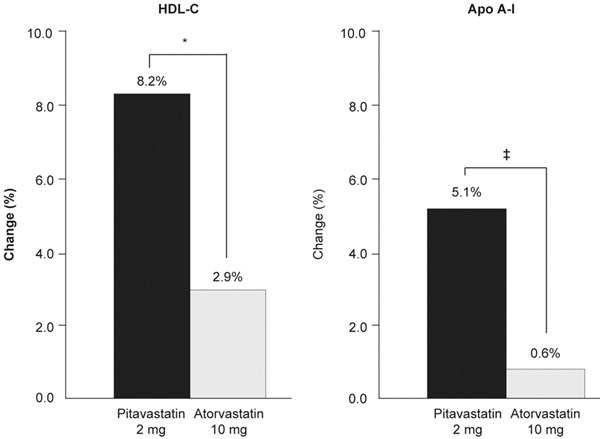
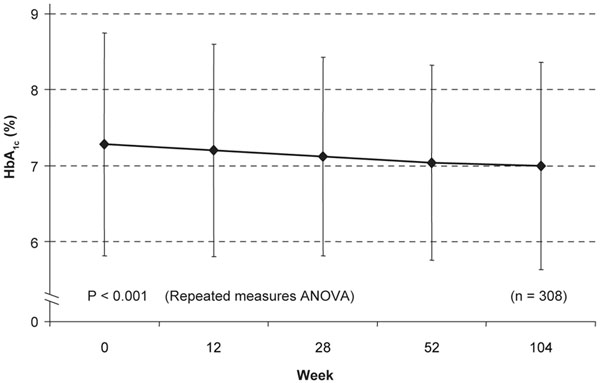
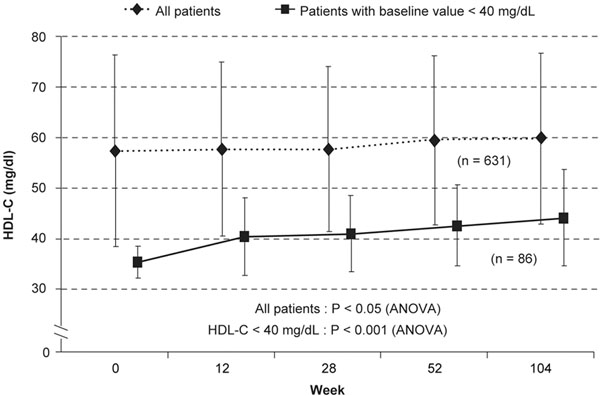
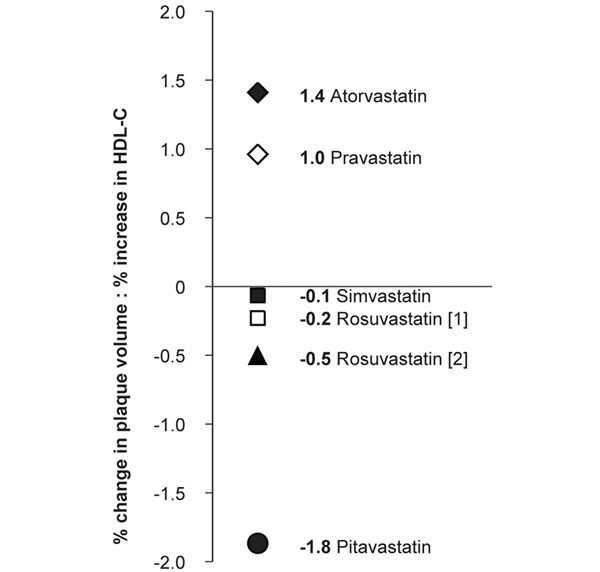
Statins effectively lower low-density lipoprotein-cholesterol (LDL-C) and reduce cardiovascular risk in people with dyslipidemia and cardiometabolic diseases such as Metabolic syndrome (MetS) or type 2 diabetes (T2D). In addition to elevated levels of LDL-C, people with these conditions often have other lipid-related risk factors, such as high levels of triglycerides, low levels of high-density lipoprotein-cholesterol (HDL-C), and a preponderance of highly atherogenic, small, dense low-density lipoprotein particles. The optimal management of dyslipidemia in people with MetS or T2D should therefore address each of these risk factors in addition to LDL-C. Although statins typically have similar effects on LDL-C levels, differences in chemical structure and pharmacokinetic profile can lead to variations in pleiotropic effects, adverse event profiles and drug-drug interactions. The choice of statin should therefore depend on the characteristics and needs of the individual patient. Compared with other statins, pitavastatin has distinct pharmacological features that translate into a broad range of actions on both apolipoprotein-B-containing and apolipoprotein-A-containing lipoproteins. Studies show that pitavastatin 1 to 4 mg is well tolerated and significantly improves LDL-C and triglyceride levels to a similar or greater degree than comparable doses of atorvastatin, simvastatin or pravastatin, irrespective of diabetic status. Moreover, whereas most statins show inconsistent effects on HDL-C levels, pitavastatin-treated patients routinely experience clinically significant elevations in HDL-C that are maintained and even increased over the long term. In addition to increasing high-density lipoprotein quantity, pitavastatin appears to improve high-density lipoprotein function and to slow the progression of atherosclerotic plaques by modifying high-density lipoprotein-related inflammation and oxidation, both of which are common in patients with MetS and T2D. When choosing a statin, it is important to note that patients with MetS have an increased risk of developing T2D and that some statins can exacerbate this risk via adverse effects on glucose regulation. Unlike many statins, pitavastatin appears to have a neutral and even beneficial effect on glucose regulation, making it a useful treatment option in this high-risk group of patients. Together with pitavastatin's beneficial effects on the cardiometabolic lipid profile and its low potential for drug-drug interactions, this suggests that pitavastatin might be a useful lipid-lowering option for people with cardiometabolic disease.
他汀类药物能有效降低低密度脂蛋白胆固醇(LDL-C),并降低血脂异常以及代谢综合征(MetS)或 2 型糖尿病(T2D)等心血管代谢疾病患者的心血管风险。除了 LDL-C 水平升高外,这些患者通常还有其他与脂质相关的危险因素,如甘油三酯水平升高、高密度脂蛋白胆固醇(HDL-C)水平降低以及富含高度动脉粥样硬化性、小而密的 LDL 颗粒。因此,代谢综合征或 2 型糖尿病患者的血脂异常最佳管理应除了 LDL-C 外,还应针对这些危险因素。尽管他汀类药物通常对 LDL-C 水平具有相似的作用,但化学结构和药代动力学特征的差异可导致多效性作用、不良事件谱和药物相互作用的差异。因此,他汀类药物的选择应取决于个体患者的特征和需求。与其他他汀类药物相比,匹伐他汀具有独特的药理学特征,可广泛作用于载脂蛋白 B 含脂蛋白和载脂蛋白 A 含脂蛋白。研究表明,匹伐他汀 1 至 4mg 具有良好的耐受性,可显著降低 LDL-C 和甘油三酯水平,其效果与阿托伐他汀、辛伐他汀或普伐他汀的可比剂量相似或更优,而与糖尿病状态无关。此外,虽然大多数他汀类药物对 HDL-C 水平的影响不一致,但匹伐他汀治疗的患者通常会经历 HDL-C 的临床显著升高,且在长期内保持甚至增加。除了增加高密度脂蛋白数量外,匹伐他汀似乎还通过改变与高密度脂蛋白相关的炎症和氧化来改善高密度脂蛋白的功能并减缓动脉粥样硬化斑块的进展,这在代谢综合征和 2 型糖尿病患者中很常见。选择他汀类药物时,需要注意的是,代谢综合征患者发生 2 型糖尿病的风险增加,而一些他汀类药物可能会通过对葡萄糖调节的不良影响而加重这种风险。与许多他汀类药物不同,匹伐他汀似乎对葡萄糖调节具有中性甚至有益的影响,使其成为这群高危患者的一种有用治疗选择。匹伐他汀对心血管代谢脂质谱的有益影响及其与药物相互作用的低潜力表明,匹伐他汀可能是心血管代谢疾病患者降低血脂的有效选择。