Barbara Davis Center for Childhood Diabetes, University of Colorado Denver, Aurora, Colorado, USA.
Diabetes Care. 2013 Sep;36(9):2607-14. doi: 10.2337/dc12-2538. Epub 2013 Jul 8.
To determine whether baseline estimated glomerular filtration rate (eGFR) and albumin-to-creatinine ratio (ACR) independently predict coronary artery calcification (CAC) progression, and to determine how eGFR changes over 6 years in adults with type 1 diabetes compared with nondiabetic adults.
The Coronary Artery Calcification in Type 1 Diabetes study participants (n = 1,066) with complete data for eGFR assessment at baseline and 6 years were included. Three Chronic Kidney Disease Epidemiology Collaboration equations (serum creatinine, cystatin C, and both) were used to estimate eGFR. The association of baseline ACR and eGFR with CAC progression was analyzed using multiple logistic regression.
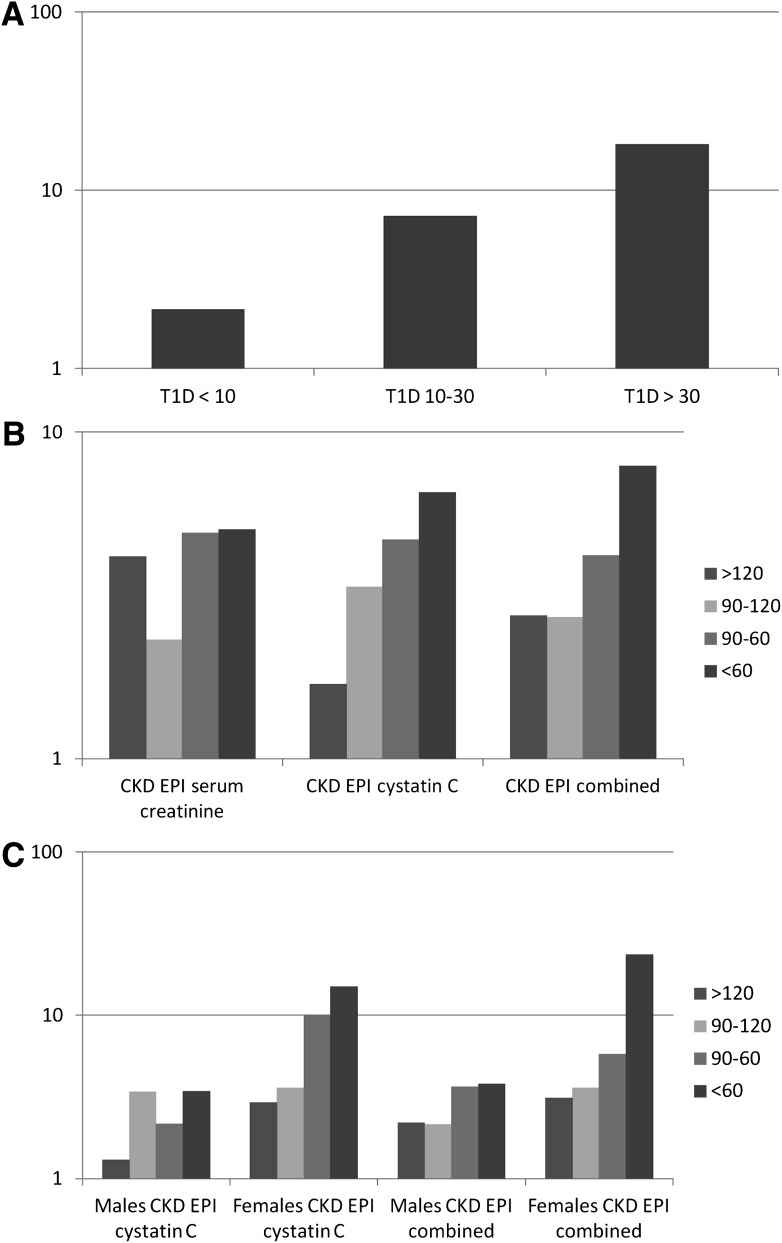
Increasing categorical baseline ACR (<10, 10-30, and >30 µg/mg) predicted CAC progression in participants with type 1 diabetes (odds ratio [OR], 2.15; 95% CI, 1.50-3.09; 7.19 [3.90-13.26]; and 18.09 [8.48-38.62]), respectively, compared with nondiabetic subjects. Baseline eGFR <60 mL/min/1.73 m(2) also predicted CAC progression (OR, 5-7, compared with nondiabetic participants). ORs for CAC progression were higher in women than in men when using the cystatin C-based Chronic Kidney Disease Epidemiology Collaboration equations. Participants with type 1 diabetes had greater eGFR decreases over 6 years than nondiabetic participants using cystatin C-based equations.
Although increasing ACR or decreasing eGFR predicts CAC progression, coronary atherosclerosis progresses faster in people with type 1 diabetes even in the absence of diabetic kidney disease. These findings emphasize the interaction between kidney disease and cardiovascular disease in type 1 diabetes and highlight the public health importance of lowering cardiorenal risk in people with type 1 diabetes.
确定基线估算肾小球滤过率(eGFR)和白蛋白与肌酐比值(ACR)是否独立预测冠状动脉钙化(CAC)进展,并确定 1 型糖尿病成人与非糖尿病成人相比,6 年内 eGFR 的变化情况。
本研究纳入了冠状动脉钙化在 1 型糖尿病研究(n=1066)中基线和 6 年时 eGFR 评估数据完整的参与者。使用 3 种慢性肾脏病流行病学合作组方程(血清肌酐、胱抑素 C 和两者)来估计 eGFR。使用多因素逻辑回归分析基线 ACR 和 eGFR 与 CAC 进展的相关性。
与非糖尿病受试者相比,1 型糖尿病患者中,递增的基线 ACR(<10、10-30 和>30 µg/mg)分别预测 CAC 进展(比值比[OR],2.15;95%可信区间[CI],1.50-3.09;7.19 [3.90-13.26];18.09 [8.48-38.62])。基线 eGFR <60 mL/min/1.73 m(2) 也预测 CAC 进展(OR,5-7,与非糖尿病参与者相比)。使用基于胱抑素 C 的慢性肾脏病流行病学合作组方程时,女性的 CAC 进展 OR 高于男性。与非糖尿病参与者相比,1 型糖尿病患者使用基于胱抑素 C 的方程时,eGFR 在 6 年内下降幅度更大。
尽管 ACR 升高或 eGFR 降低预测 CAC 进展,但即使在没有糖尿病肾病的情况下,1 型糖尿病患者的冠状动脉粥样硬化进展更快。这些发现强调了 1 型糖尿病中肾脏疾病和心血管疾病之间的相互作用,并突出了降低 1 型糖尿病患者心肾风险的重要性。