Department of Cardiovascular Sciences, Research Unit of Experimental Cardiac Surgery, KU Leuven, Herestraat 49, Leuven B-3000, Belgium.
BMC Cardiovasc Disord. 2013 Jul 12;13:51. doi: 10.1186/1471-2261-13-51.
Diabetic cardiomyopathy is characterized by systolic and early diastolic ventricular dysfunction. In the metabolic syndrome (MS), ventricular stiffness is additionally increased in a later stage. It is unknown whether this is related to intrinsic cardiomyocyte dysfunction, extrinsic factors influencing cardiomyocyte contractility and/or cardiac function, or a combination of both. A first aim was to study cardiomyocyte contractility and Ca2+ handling in vitro in a mouse model of MS. A second aim was to investigate whether in vivo hypocaloric diet or ACE-inhibition (ACE-I) improved cardiomyocyte contractility in vitro, contractile reserve and Ca2+ handling.
This study was performed in LDL-receptor (LDLR-/-) and leptin-deficient (ob/ob), double knock-out mice (DKO), featuring obesity, type II diabetes, atherogenic dyslipidemia and hypertension. Single knock-out LDLR-/-, ob/ob and wild type mice were used as controls. Cellular contractility, Ca2+ handling and their response to in vivo treatment with diet or ACE-I were studied in isolated cardiomyocytes at baseline, during β-adrenergic stimulation or increased extracellular Ca2+, using field stimulation and patch-clamp.
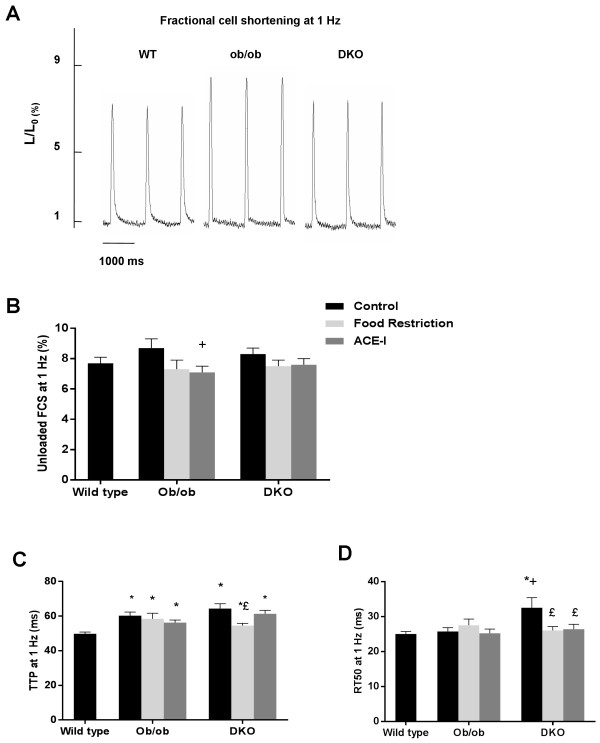
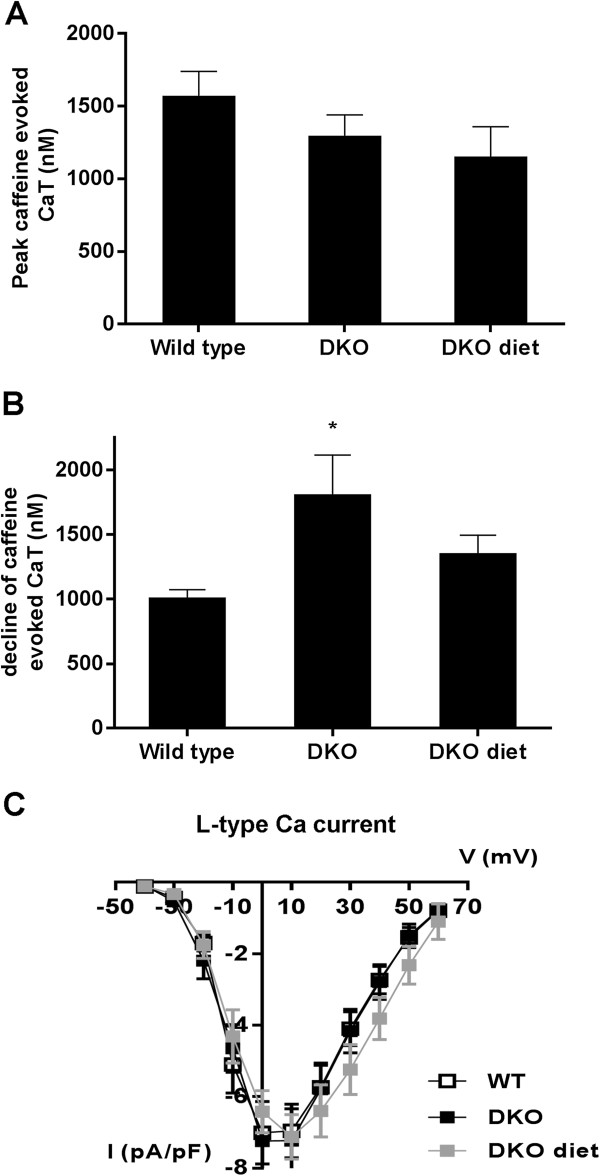
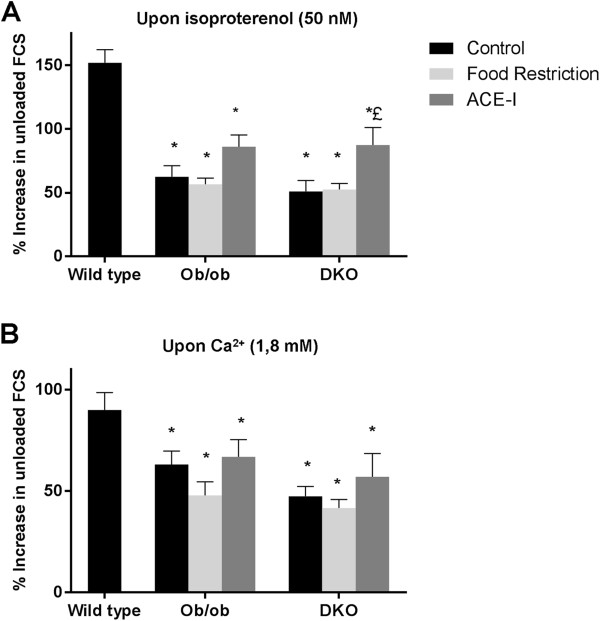
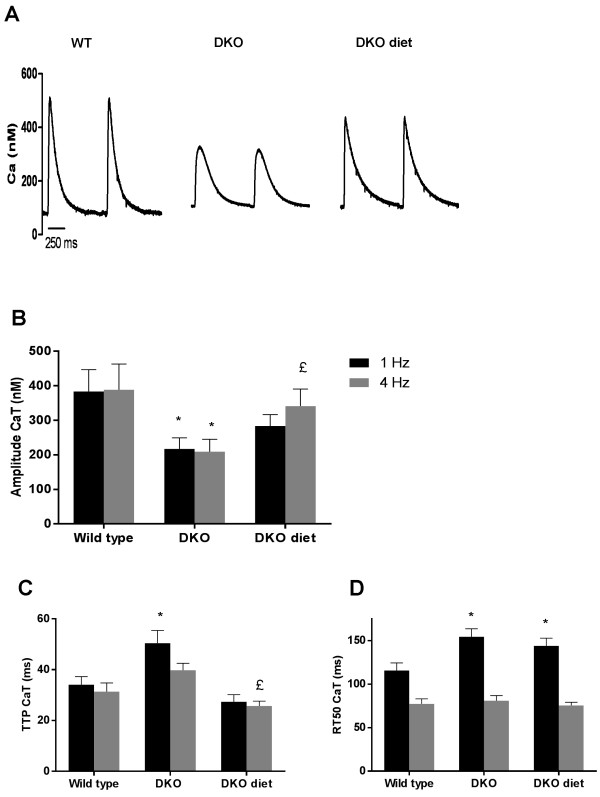
In untreated conditions, prolongation of contraction-relaxation cycle and altered Ca2+ handling are observed in MS. Response to increased extracellular Ca2+ and β-adrenergic stimulation is impaired and could not be rescued by weight loss. ACE-I restored impaired response to β-adrenergic stimulation in MS, but not the decreased response to increased extracellular Ca2+.
Cardiomyocyte contractility and β-adrenergic response are impaired in MS, due to alterations in cellular Ca2+ handling. ACE-I, but not weight loss, is able to restore cardiomyocyte response to β-adrenergic stimulation in MS.
糖尿病心肌病的特征是收缩期和舒张早期心室功能障碍。在代谢综合征(MS)中,心室僵硬度在后期进一步增加。目前尚不清楚这是否与内在心肌细胞功能障碍、影响心肌细胞收缩性和/或心功能的外在因素有关,或者是两者的结合。第一个目的是在 MS 的小鼠模型中研究体外心肌细胞的收缩性和 Ca2+处理。第二个目的是研究体内低热量饮食或 ACE 抑制剂(ACE-I)是否能改善体外心肌细胞的收缩性、收缩储备和 Ca2+处理。
本研究在 LDL 受体(LDLR-/-)和瘦素缺乏(ob/ob)、双敲除(DKO)小鼠中进行,这些小鼠表现出肥胖、II 型糖尿病、动脉粥样硬化性血脂异常和高血压。单敲除 LDLR-/-, ob/ob 和野生型小鼠作为对照。在基础状态、β-肾上腺素能刺激或增加细胞外 Ca2+时,使用场刺激和膜片钳技术,在分离的心肌细胞中研究细胞收缩性、Ca2+处理及其对体内饮食或 ACE-I 治疗的反应。
在未经治疗的情况下,MS 中观察到收缩-舒张周期延长和 Ca2+处理改变。对增加的细胞外 Ca2+和β-肾上腺素能刺激的反应受损,并且不能通过减肥来挽救。ACE-I 恢复了 MS 中受损的β-肾上腺素能刺激反应,但不能恢复对增加的细胞外 Ca2+的反应。
MS 中的心肌细胞收缩性和β-肾上腺素能反应受损,原因是细胞内 Ca2+处理发生改变。ACE-I,但不是减肥,能够恢复 MS 中β-肾上腺素能刺激反应的心肌细胞。