Azienda Ospedaliera Universitaria Integrata di Verona, FISH Molecular Laboratory, Department of Pathology and Diagnostic, University of Verona, Verona, Italy.
PLoS One. 2013 Jul 10;8(7):e68203. doi: 10.1371/journal.pone.0068203. Print 2013.
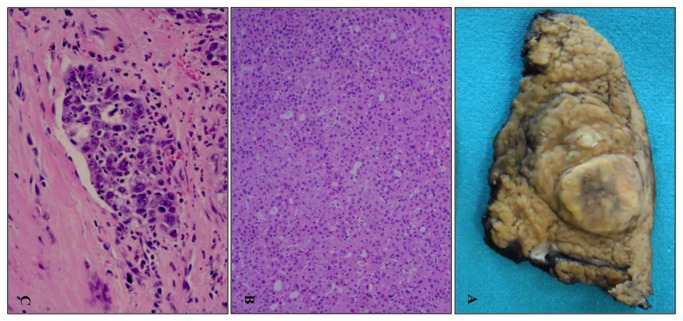
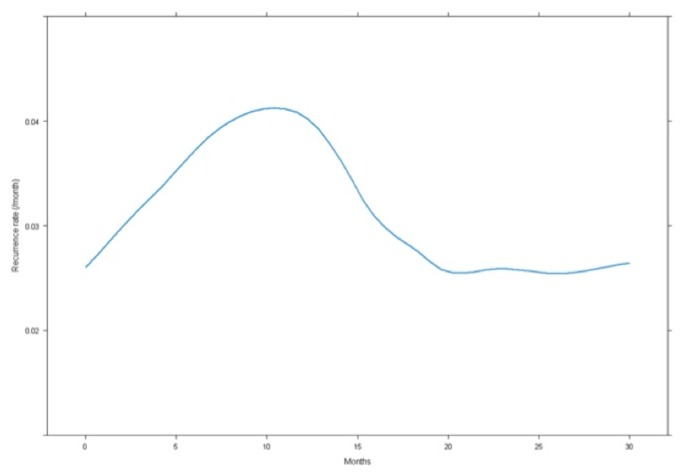
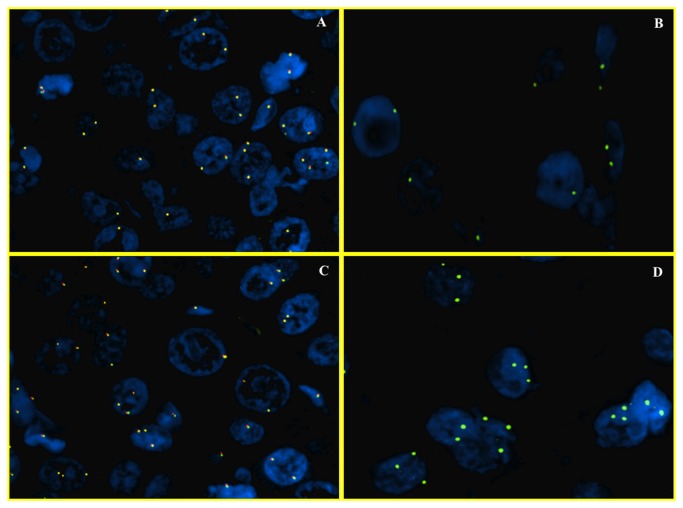
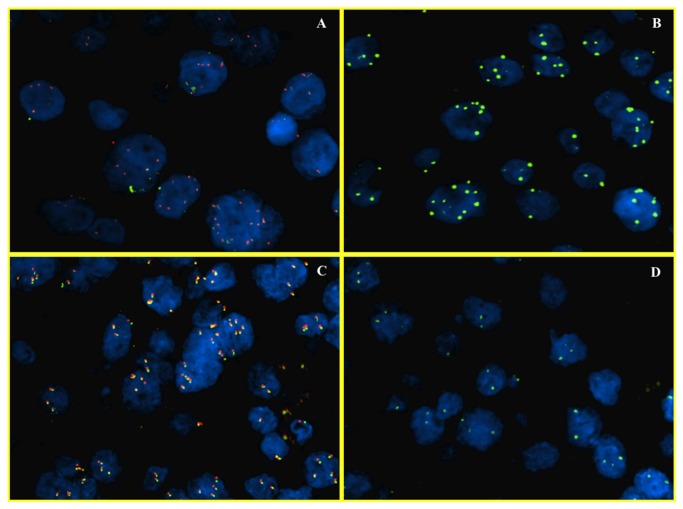
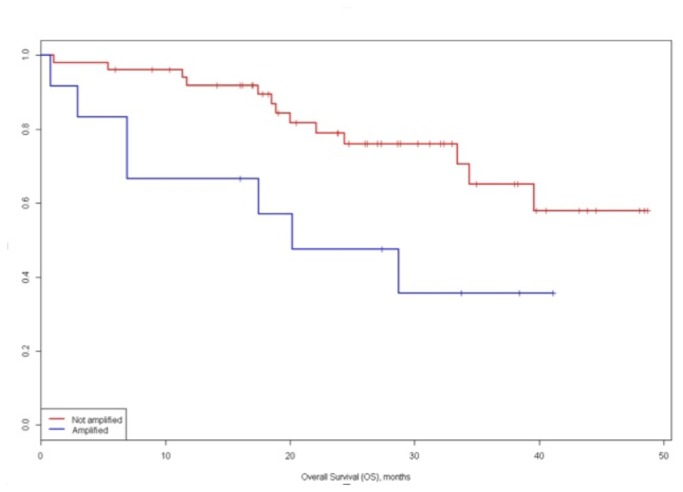
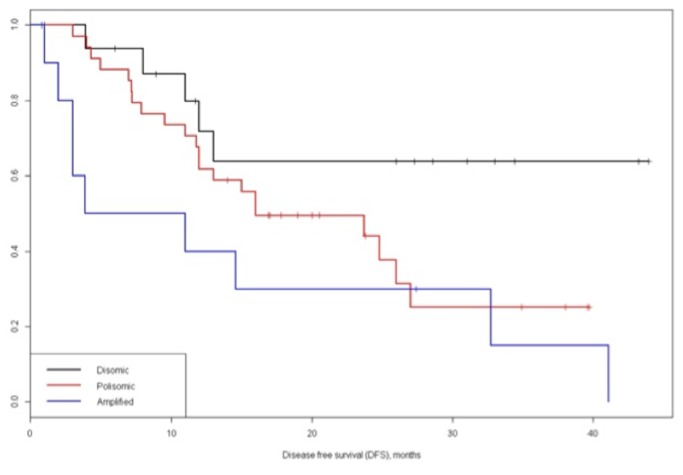
Hepatocellular carcinoma is one leading cause of cancer-related death and surgical resection is still one of the major curative therapies. Recently, there has been a major effort to find mechanisms involved in carcinogenesis and early relapse. c-myc gene abnormality is found in hepatocarcinogenesis. Our aim was to analyze the role of c-myc as prognostic factor in terms of overall survival and disease-free survival and to investigate if c-myc may be an important target for therapy. We studied sixty-five hepatocellular carcinomas submitted to surgical resection with curative intent. Size, macro-microvascular invasion, necrosis, number of nodules, grading and serum alfa-fetoprotein level were registered for all cases. We evaluated the c-myc aberrations by using break-apart FISH probes. Probes specific for the centromeric part of chromosome 8 and for the locus specific c-myc gene (8q24) were used to assess disomy, gains of chromosomes (polysomy due to polyploidy) and amplification. c-myc gene amplification was scored as 8q24/CEP8 > 2. Statistical analysis for disease-free survival and overall survival were performed. At molecular level, c-myc was amplified in 19% of hepatocellular carcinoma, whereas showed gains in 55% and set wild in 26% of cases. The 1- and 3-year disease-free survival and overall survival for disomic, polysomic and amplified groups were significantly different (p=0.020 and p=.018 respectively). Multivariate analysis verified that the AFP and c-myc status (amplified vs. not amplified) were significant prognostic factors for overall patients survival. c-myc gene amplification is significantly correlated with disease-free survival and overall survival in patients with hepatocellular carcinoma after surgical resection and this model identifies patients with risk of early relapse (≤12 months). We suggest that c-myc assessment may be introduced in the clinical practice for improving prognostication (high and low risk of relapse) routinely and may have be proposed as biomarker of efficacy to anti-c-myc targeted drugs in clinical trials.
肝细胞癌是癌症相关死亡的主要原因之一,手术切除仍然是主要的治愈性治疗方法之一。最近,人们一直在努力寻找与癌变和早期复发相关的机制。在肝癌发生过程中发现 c-myc 基因异常。我们的目的是分析 c-myc 作为总生存和无病生存的预后因素,并探讨 c-myc 是否可能成为治疗的重要靶点。我们研究了 65 例接受根治性手术切除的肝细胞癌。所有病例均记录肿瘤大小、巨微脉管侵犯、坏死、结节数、分级和血清甲胎蛋白水平。我们使用断裂分离 FISH 探针评估 c-myc 异常。使用针对染色体 8 着丝粒部分和 8q24 基因座特异性 c-myc 基因的探针来评估非整倍体、染色体获得(多倍体引起的多倍体)和扩增。c-myc 基因扩增评分 8q24/CEP8>2。对无病生存和总生存进行统计分析。在分子水平上,c-myc 在 19%的肝细胞癌中扩增,在 55%的病例中获得,在 26%的病例中野生。非整倍体、多倍体和扩增组的 1 年和 3 年无病生存率和总生存率差异有统计学意义(p=0.020 和 p=0.018)。多因素分析证实 AFP 和 c-myc 状态(扩增与未扩增)是总体患者生存的显著预后因素。c-myc 基因扩增与肝细胞癌患者手术后的无病生存和总生存显著相关,该模型可识别早期复发(≤12 个月)风险患者。我们建议,c-myc 评估可引入临床实践,以常规改善预后(复发风险高和低),并可能作为临床试验中抗 c-myc 靶向药物疗效的生物标志物。