Malaria Branch, KEMRI/CDC Research and Public Health Collaboration, Kisumu, Kenya.
PLoS One. 2013 Jul 16;8(7):e68733. doi: 10.1371/journal.pone.0068733. Print 2013.
Pregnancy-related (PR) deaths are often a result of direct obstetric complications occurring at childbirth.
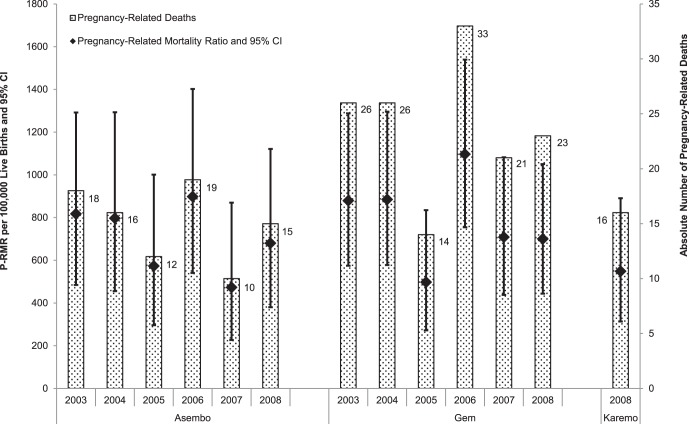
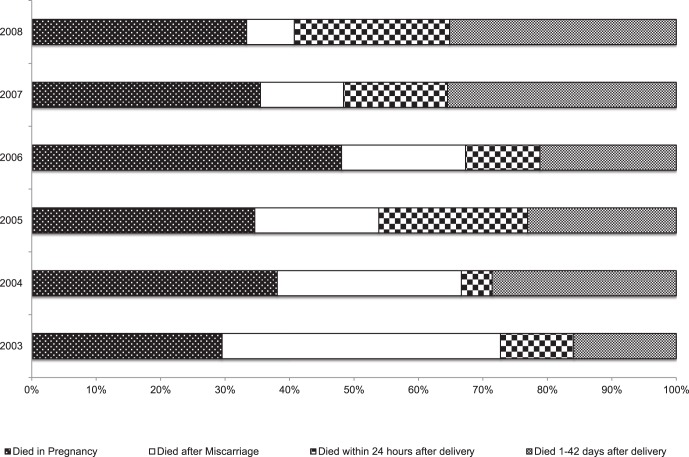
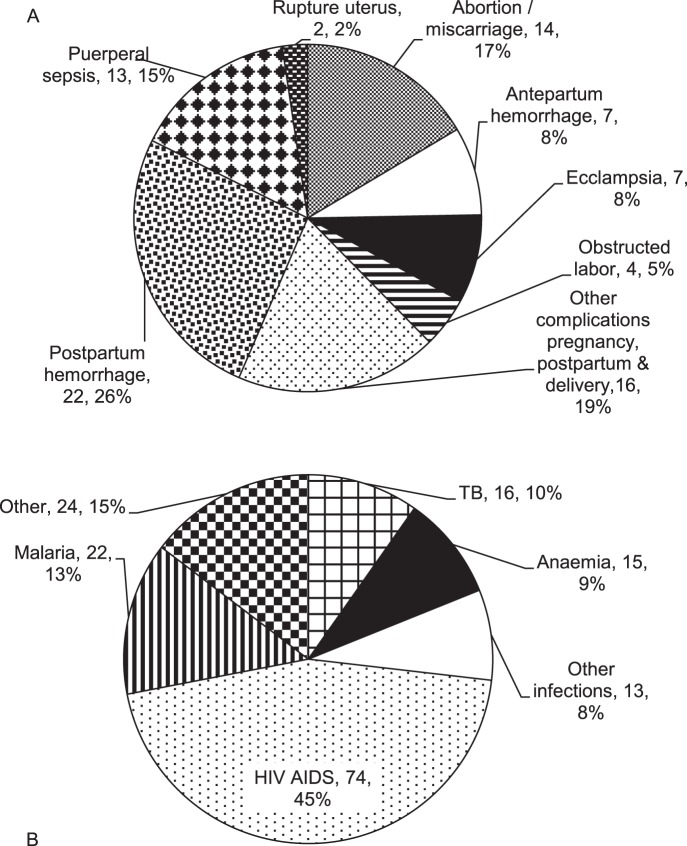
To estimate the burden of and characterize risk factors for PR mortality, we evaluated deaths that occurred between 2003 and 2008 among women of childbearing age (15 to 49 years) using Health and Demographic Surveillance System data in rural western Kenya. WHO ICD definition of PR mortality was used: "the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death". In addition, symptoms and events at the time of death were examined using the WHO verbal autopsy methodology. Deaths were categorized as either (i) directly PR: main cause of death was ascribed as obstetric, or (ii) indirectly PR: main cause of death was non-obstetric. Of 3,223 deaths in women 15 to 49 years, 249 (7.7%) were PR. One-third (34%) of these were due to direct obstetric causes, predominantly postpartum hemorrhage, abortion complications and puerperal sepsis. Two-thirds were indirect; three-quarters were attributable to human immunodeficiency virus (HIV/AIDS), malaria and tuberculosis. Significantly more women who died in lower socio-economic groups sought care from traditional birth attendants (p = 0.034), while less impoverished women were more likely to seek hospital care (p = 0.001). The PR mortality ratio over the six years was 740 (95% CI 651-838) per 100,000 live births, with no evidence of reduction over time (χ(2) linear trend = 1.07; p = 0.3).
These data supplement current scanty information on the relationship between infectious diseases and poor maternal outcomes in Africa. They indicate low uptake of maternal health interventions in women dying during pregnancy and postpartum, suggesting improved access to and increased uptake of skilled obstetric care, as well as preventive measures against HIV/AIDS, malaria and tuberculosis among all women of childbearing age may help to reduce pregnancy-related mortality.
妊娠相关(PR)死亡通常是分娩时直接产科并发症的结果。
为了估计 PR 死亡率的负担并描述其危险因素,我们使用肯尼亚西部农村地区的健康和人口监测系统数据,评估了 2003 年至 2008 年间生育年龄(15 至 49 岁)的妇女的死亡情况。采用世卫组织对 PR 死亡率的 ICD 定义:“孕妇或妊娠终止后 42 天内死亡的妇女,无论死亡原因如何”。此外,还使用世卫组织的死因推断法检查了死亡时的症状和事件。死亡分为直接 PR:主要死因归因于产科,或间接 PR:主要死因是非产科。在 15 至 49 岁的妇女中,有 3223 人死亡,其中 249 人(7.7%)是 PR。其中三分之一(34%)是由直接产科原因引起的,主要是产后出血、流产并发症和产褥期败血症。三分之二是间接的;四分之三归因于人类免疫缺陷病毒(HIV/AIDS)、疟疾和结核病。明显更多处于较低社会经济群体的妇女寻求传统助产妇的护理(p=0.034),而贫困程度较低的妇女更有可能寻求医院护理(p=0.001)。六年期间 PR 死亡率为每 100000 例活产 740(95%CI651-838),没有随着时间的推移而减少的证据(χ(2)线性趋势=1.07;p=0.3)。
这些数据补充了目前关于非洲传染病与不良产妇结局之间关系的稀缺信息。它们表明,在妊娠和产后期间死亡的妇女中,接受母婴保健干预的人数较少,这表明需要改善所有生育年龄妇女获得熟练产科护理的机会,并增加接受率,以及采取预防艾滋病毒/艾滋病、疟疾和结核病的措施,以帮助降低妊娠相关死亡率。