Department of Respiratory Medicine, Saitama Medical University, Saitama, Japan.
BMJ Open. 2013 Jul 31;3(7):e002971. doi: 10.1136/bmjopen-2013-002971.
To assess clinical, laboratory and radiographic findings associated with outcomes and to clarify more practical ways to predict hospital mortality in patients with acute exacerbation (AE) of chronic fibrosing interstitial pneumonia (CFIP).
Single-centre retrospective cohort study.
University Hospital in Japan.
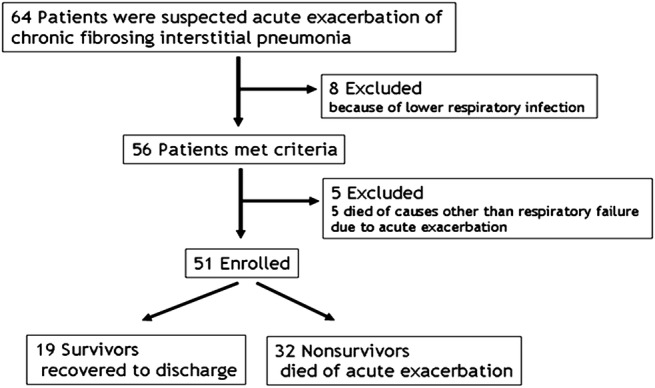
We identified 51 consecutive patients with AE of idiopathic CFIP through multidisciplinary discussion. Patients who had connective tissue disease, drug-induced lung disease, pneumoconiosis, hypersensitivity pneumonitis, sarcoidosis, pulmonary histiocytosis, lymphangioleiomyomatosis and eosinophilic pneumonia were excluded.
There were no interventions.
The main outcome was determination of in-hospital mortality predictors. Other outcomes included clinical, laboratory and radiographic differences between non-survivors and survivors in patients with AE of CFIP.
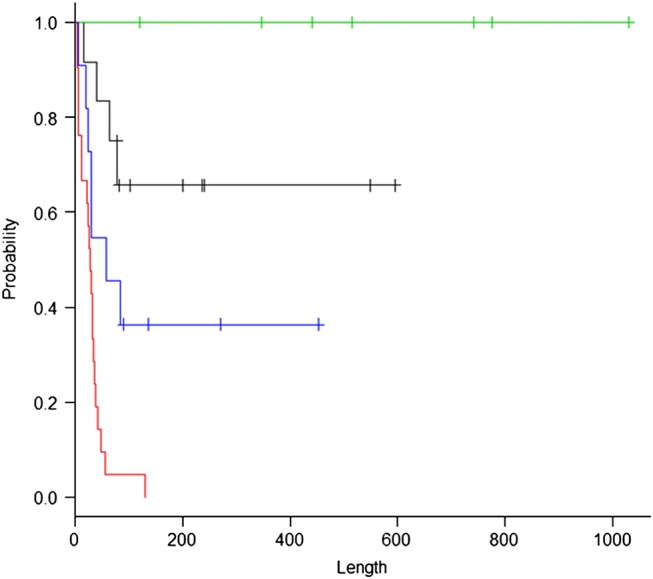
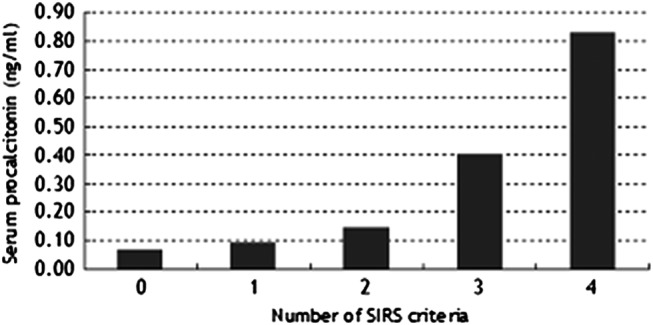
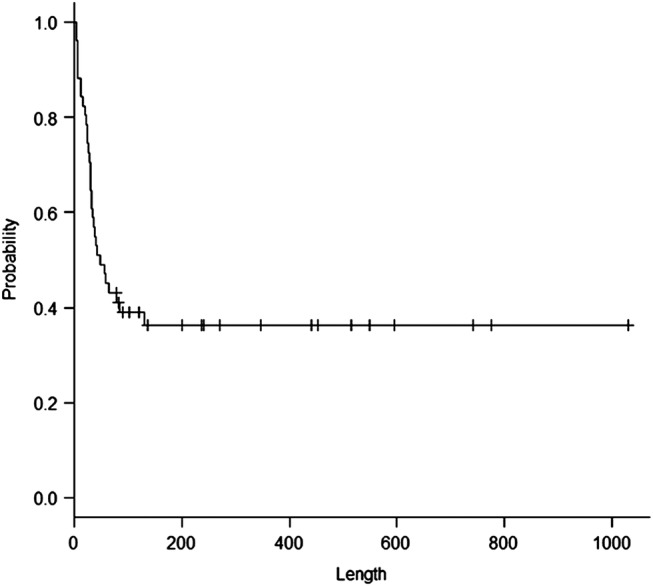
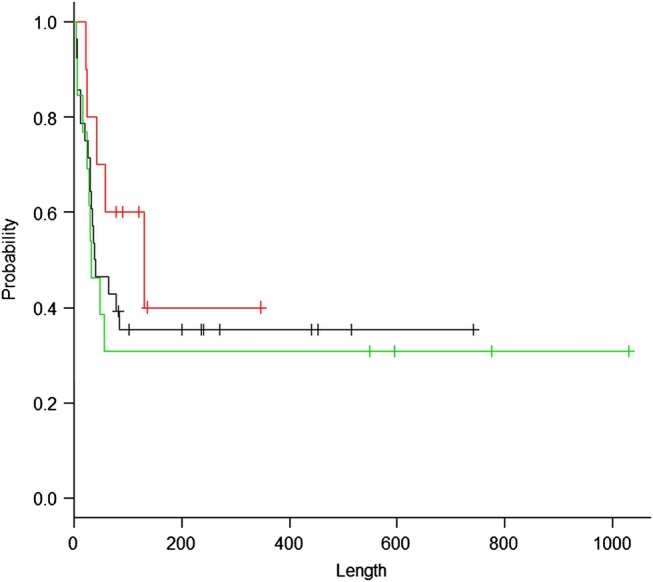
The mean age of the patients with AE of CFIP was 71 years. Compared with survivors, non-survivors had a significantly shorter duration of symptoms before admission, lower prevalence of peripheral distribution of ground-glass opacity and centrilobular emphysema (CLE) on thin-section CT, lower peripheral lymphocyte count, higher brain natriuretic peptide titre, lower Pao2:Fio2 (P:F) ratio, higher prevalence of systemic inflammatory response syndrome (SIRS) and higher SIRS score on admission (p=0.0069, 0.0032, 0.015, 0.040, 0.0098, 0.012, 9.9×10(-7) and 5.4×10(-6), respectively). Multivariate analysis revealed SIRS (HR=6.2810, p=0.015), CLE (HR=0.0606, p=3.6×10(-5)) and serum procalcitonin level (HR=2.7110, p=0.022) to be independent predictors of in-hospital mortality. A Kaplan-Meier estimate on the basis of stratification according to the presence or absence of SIRS and CLE demonstrated a distinct survival curve for each subset of patients.
Distinct survival curves documented by stratification according to the presence or absence of SIRS and CLE may provide basic information for a rational management strategy for patients with AE of CFIP on admission.
评估与结局相关的临床、实验室和影像学发现,并阐明更实用的方法来预测慢性纤维化间质性肺炎(CFIP)急性加重(AE)患者的住院死亡率。
单中心回顾性队列研究。
日本大学医院。
通过多学科讨论,我们确定了 51 例特发性 CFIP 的 AE 连续患者。排除患有结缔组织疾病、药物性肺病、尘肺、过敏性肺炎、结节病、淋巴管平滑肌瘤病和嗜酸性肺炎的患者。
无干预措施。
住院死亡率预测因素的确定。其他结局包括 CFIP AE 患者中存活者与非存活者之间临床、实验室和影像学的差异。
CFIP AE 患者的平均年龄为 71 岁。与存活者相比,非存活者入院前症状持续时间明显更短,磨玻璃影和小叶中心性肺气肿(CLE)在薄层 CT 上的外周分布更少见,外周淋巴细胞计数更低,脑利钠肽水平更高,动脉血氧分压/吸入氧浓度(P/F)比值更低,入院时全身炎症反应综合征(SIRS)和 SIRS 评分更高(p=0.0069、0.0032、0.015、0.040、0.0098、0.012、9.9×10(-7)和 5.4×10(-6),分别)。多变量分析显示 SIRS(HR=6.2810,p=0.015)、CLE(HR=0.0606,p=3.6×10(-5))和血清降钙素原水平(HR=2.7110,p=0.022)是住院死亡率的独立预测因素。根据是否存在 SIRS 和 CLE 进行分层的 Kaplan-Meier 估计表明,每个患者亚组的生存曲线明显不同。
根据 SIRS 和 CLE 的存在与否进行分层记录的明显生存曲线可为 CFIP AE 患者入院时的合理管理策略提供基础信息。