Division of Medical Genetics, A. I. duPont Hospital for Children, Wilmington, Delaware.
Am J Med Genet A. 2013 Oct;161A(10):2420-30. doi: 10.1002/ajmg.a.36098. Epub 2013 Aug 5.
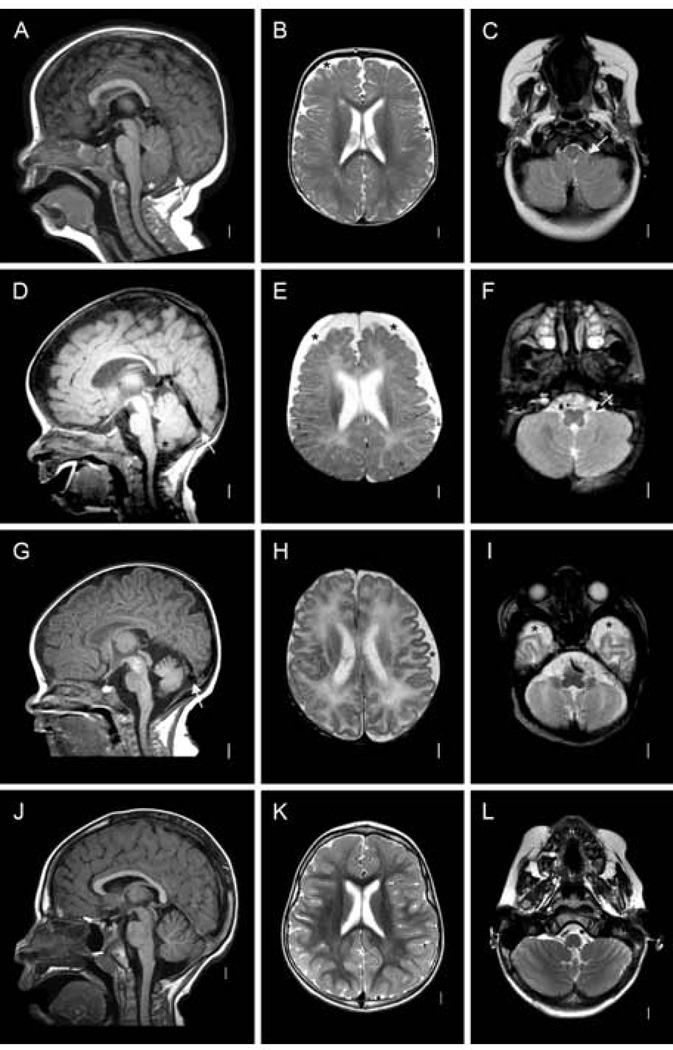
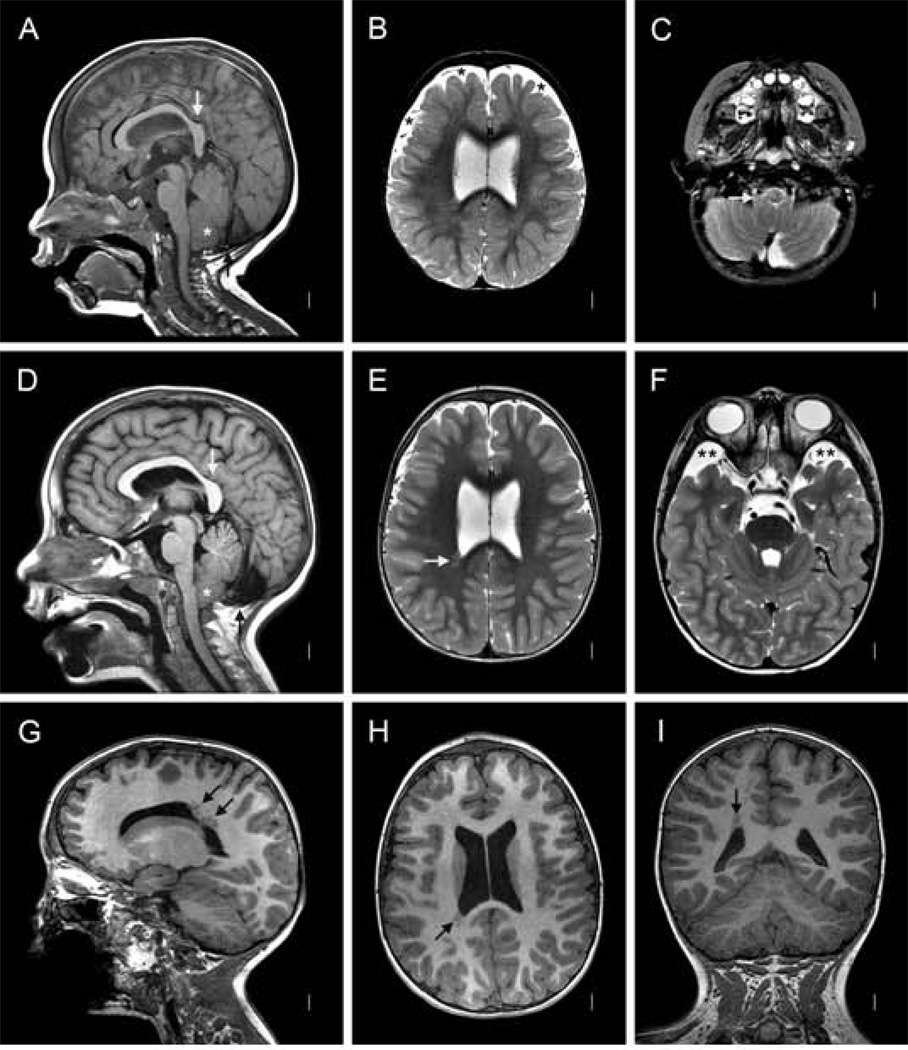
Noonan syndrome is a heterogenous rasopathy typically presenting with short stature, characteristic facial features, cardiac abnormalities including pulmonic valve stenosis, ASD and hypertrophic cardiomyopathy (HCM), cryptorchidism, ectodermal abnormalities, and learning differences. The phenotype is variable, and limited genotype phenotype correlation exists with SOS1 mutations often associated with normal cognition and stature, RAF1 mutations entailing a high HCM risk, and certain PTPN11 mutations predisposing to juvenile myelomonocytic leukemia. The recently identified SHOC2 mutation (p.Ser2Gly) causes Noonan syndrome with loose anagen hair. We report five patients with this mutation. All had skin hyperpigmentation, sparse light colored hair, increased fine wrinkles, ligamentous laxity, developmental delay, and 4/4 had a structural cardiac anomaly. Hypotonia and macrocephaly occurred in 4/5 (80%); 3/5 (60%) had polyhydramnios, increased birth weight or required use of a feeding tube. Distinctive brain abnormalities included relative megalencephaly and enlarged subarachnoid spaces suggestive of benign external hydrocephalus, and a relatively small posterior fossa as indicated by a vertical tentorium. The combination of a large brain with a small posterior fossa likely resulted in the high rate of cerebellar tonsillar ectopia (3/4; 75%). Periventricular nodular heterotopia was seen in one patient with a thick and dysplastic corpus callosum. We report on the first hematologic neoplasm, myelofibrosis, in a 2-year-old patient with SHOC2 mutation. Myelofibrosis is exceedingly rare in children and young adults. The absence of a somatic JAK2 mutation, seen in the majority of patients with myelofibrosis, is noteworthy as it suggests that germline or somatic SHOC2 mutations are causally involved in myelofibrosis.
努南综合征是一种异质性的 Ras 病,通常表现为身材矮小、特征性面部特征、心脏异常,包括肺动脉瓣狭窄、房间隔缺损和肥厚型心肌病(HCM)、隐睾、外胚层异常和学习差异。表型具有变异性,并且 SOS1 突变与正常认知和身高相关,RAF1 突变导致 HCM 风险增加,某些 PTPN11 突变易导致青少年骨髓单核细胞白血病,其基因型-表型相关性有限。最近发现的 SHOC2 突变(p.Ser2Gly)导致具有疏松生长期毛发的努南综合征。我们报告了五例这种突变的患者。所有患者均有皮肤色素沉着、稀疏浅色毛发、增加的细皱纹、韧带松弛、发育迟缓,且 4/4 例有结构性心脏异常。低张力和大头发生长在 4/5(80%)例中;3/5(60%)例有羊水过多、出生体重增加或需要使用喂养管。明显的脑部异常包括相对的巨脑和扩大的蛛网膜下腔,提示良性外部脑积水,以及较小的后颅窝,表现为垂直天幕。大脑较大与后颅窝较小相结合,可能导致小脑扁桃体异位的发生率较高(3/4;75%)。1 例患者存在厚而发育不良的胼胝体,可见脑室周围结节性异位。我们报告了首例 SHOC2 突变患者的血液学肿瘤,骨髓纤维化。骨髓纤维化在儿童和年轻成人中极为罕见。大多数骨髓纤维化患者中存在体细胞 JAK2 突变缺失,这一点值得注意,因为它表明种系或体细胞 SHOC2 突变可能与骨髓纤维化有关。