Center for Global Health and Development, Boston University, Boston, Massachusetts, USA.
PLoS One. 2013 Jul 30;8(7):e69300. doi: 10.1371/journal.pone.0069300. Print 2013.
While CD4 strongly predicts mortality on antiretroviral therapy (ART), estimates from programmatic data suffer from incomplete patient outcomes.
We conducted a pooled analysis of one-year mortality data on ART accounting for lost patients. We identified articles reporting one-year mortality by ART initiation CD4 count. We estimated the average mortality among those lost as the value that maximizes the fit of a regression of the natural log of mortality on the natural log of the imputed mean CD4 count in each band.
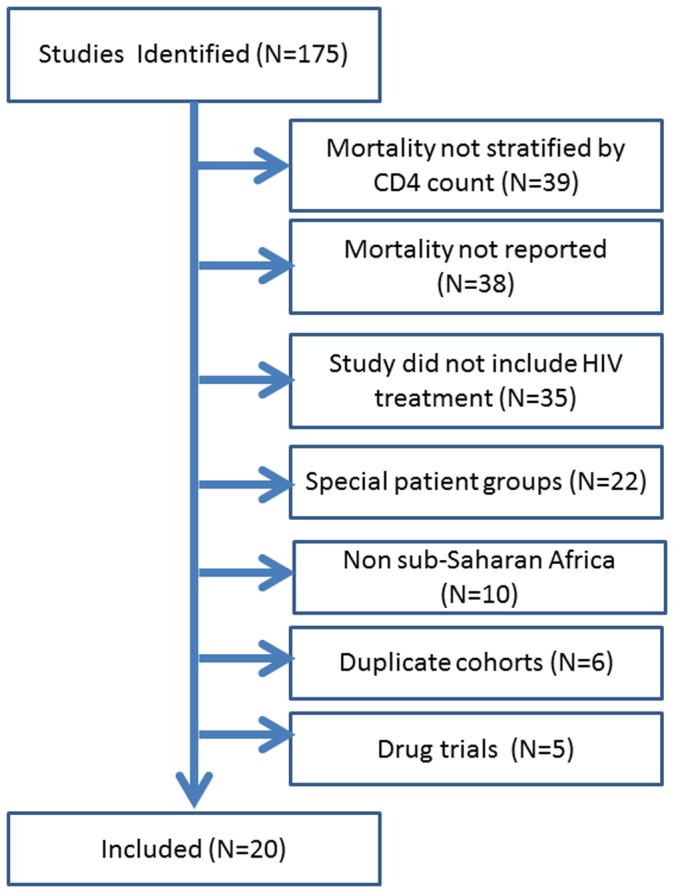
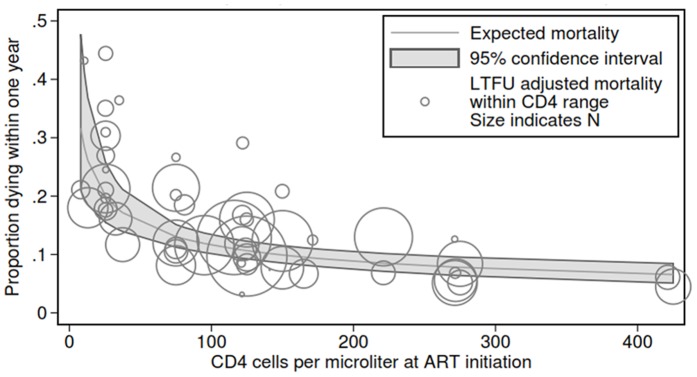
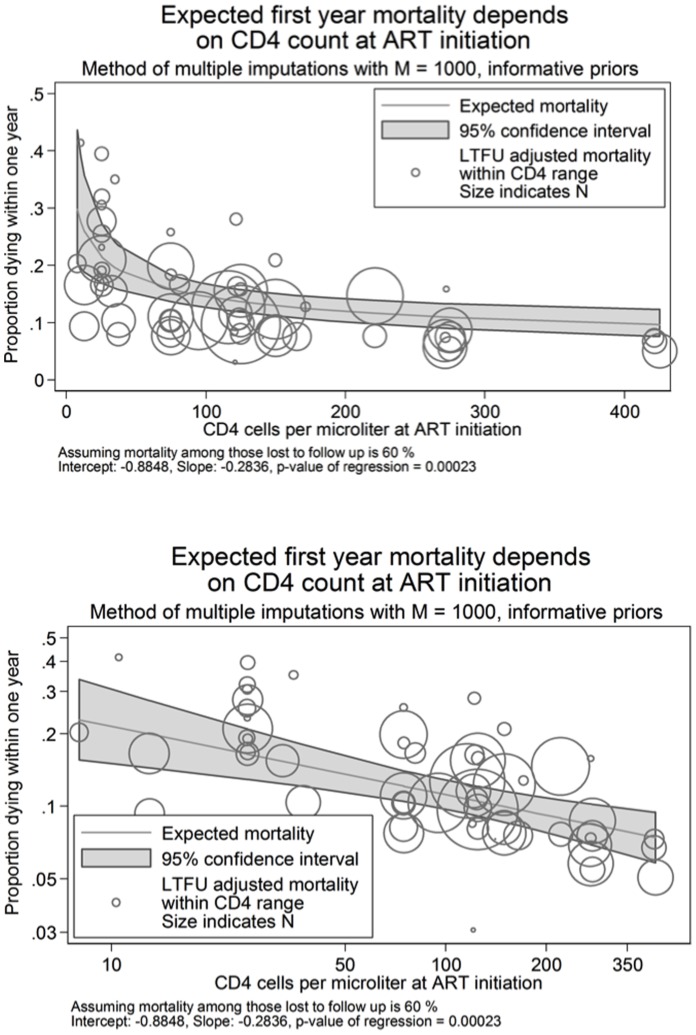
We found 20 studies representing 64,426 subjects and 51 CD4 observations. Without correcting for losses, one-year mortality was >4.8% for all CD4 counts <200 cells/mm(3). When searching over different values for mortality among those lost, the best fitting model occurs at 60% mortality. In this model, those with a CD4≤200 had a one-year mortality above 8.7, while those with a CD4>500 had a one-year mortality <6.8%. Comparing those starting ART at 500 vs. 50, one-year mortality risk was reduced by 54% (6.8 vs. 12.5%). Regardless of CD4 count, mortality was substantially higher than when assuming no mortality among those lost, ranging from a 23-94% increase.
Our best fitting regression estimates that every 10% increase in CD4 count at initiation is associated with a 2.8% decline in one-year mortality, including those lost. Our study supports the health benefits of higher thresholds for CD4 count initiation and suggests that reports of programmatic ART outcomes can and should adjust results for mortality among those lost.
CD4 强烈预测抗逆转录病毒治疗(ART)的死亡率,但来自项目数据的估计存在患者结局不完全的问题。
我们对计入失访患者的 ART 一年死亡率数据进行了汇总分析。我们检索了报告按 ART 起始 CD4 计数的一年死亡率的文章。我们将失访患者的平均死亡率估计为使死亡率的自然对数对每个 CD4 计数带的估计均值 CD4 自然对数的回归拟合最佳的值。
我们发现了 20 项研究,涉及 64426 名受试者和 51 个 CD4 观察值。未经失访校正,所有 CD4 计数<200 个细胞/mm(3)的患者一年死亡率均>4.8%。在搜索不同失访患者死亡率值时,拟合最佳的模型出现在死亡率为 60%。在该模型中,CD4≤200 的患者一年死亡率高于 8.7%,而 CD4>500 的患者一年死亡率<6.8%。与在 CD4 为 500 时开始 ART 相比,在 CD4 为 50 时开始 ART 的一年死亡率风险降低了 54%(6.8%对 12.5%)。无论 CD4 计数如何,死亡率都明显高于假设失访患者无死亡时的死亡率,增加幅度在 23%至 94%之间。
我们拟合最佳的回归估计,每 10%的 CD4 计数起始增加与一年死亡率降低 2.8%相关,包括失访患者。我们的研究支持 CD4 计数起始阈值更高的健康益处,并表明项目抗逆转录病毒治疗结果的报告可以而且应该根据失访患者的死亡率进行调整。