Department of Clinical Science Intervention and Technology, Division of Obstetrics and Gynecology, Karolinska Institutet, Stockholm, Sweden.
PLoS One. 2013 Aug 6;8(8):e70984. doi: 10.1371/journal.pone.0070984. Print 2013.
To estimate the incidence of RhD immunisation after implementation of first trimester non-invasive fetal RHD screening to select only RhD negative women carrying RHD positive fetuses for routine antenatal anti-D prophylaxis (RAADP).
We present a population-based prospective observational cohort study with historic controls including all maternity care centres and delivery hospitals in the Stockholm region, Sweden. All RhD negative pregnant women were screened for fetal RHD genotype in the first trimester of pregnancy. Anti-D immunoglobulin (250-300 µg) was administered intramuscularly in gestational week 28-30 to participants with RHD positive fetuses. Main outcome measure was the incidence of RhD immunisation developing during or after pregnancy.
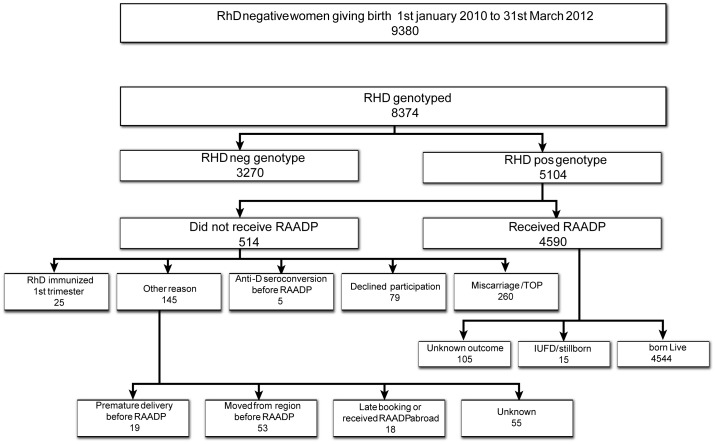
During the study period 9380 RhD negative women gave birth in Stockholm. Non-invasive fetal RHD genotyping using cell-free fetal DNA in maternal plasma was performed in 8374 pregnancies of which 5104 (61%) were RHD positive and 3270 (39%) RHD negative. In 4590 pregnancies with an RHD positive test the women received antenatal anti-D prophylaxis. The incidence of RhD immunisation in the study cohort was 0.26 percent (24/9380) (95% CI 0.15-0.36%) compared to 0.46 percent (86/18546) (95% CI 0.37 to 0.56%) in the reference cohort. The risk ratio (RR) for sensitisation was 0.55 (95% CI 0.35 to 0.87) and the risk reduction was statistically significant (p = 0.009). The absolute risk difference was 0.20 percent, corresponding to a number needed to treat (NNT) of 500.
Using first trimester non-invasive antenatal screening for fetal RHD to target routine antenatal anti-D prophylaxis selectively to RhD negative women with RHD positive fetuses significantly reduces the incidence of new RhD immunisation. The risk reduction is comparable to that reported in studies evaluating the outcome of non selective RAADP to all RhD negative women. The cost-effectiveness of this targeted approach remains to be studied.
评估在实施第一孕期非侵入性胎儿 RHD 筛检以选择仅携带 RHD 阳性胎儿的 RHD 阴性孕妇进行常规产前抗-D 预防(RAADP)后,RHD 免疫的发生率。
我们进行了一项基于人群的前瞻性观察性队列研究,包括瑞典斯德哥尔摩地区的所有产科中心和分娩医院。所有 RHD 阴性孕妇在妊娠早期接受胎儿 RHD 基因型筛查。在妊娠 28-30 周时,给携带 RHD 阳性胎儿的参与者肌内注射抗-D 免疫球蛋白(250-300μg)。主要结局指标是怀孕期间或之后发生的 RHD 免疫发生率。
在研究期间,斯德哥尔摩有 9380 名 RHD 阴性孕妇分娩。在 8374 例妊娠中使用母体血浆中的游离胎儿 DNA 进行了非侵入性胎儿 RHD 基因分型,其中 5104 例(61%)为 RHD 阳性,3270 例(39%)为 RHD 阴性。在 4590 例 RHD 阳性检测的妊娠中,妇女接受了产前抗-D 预防。研究队列的 RhD 免疫发生率为 0.26%(24/9380)(95%CI 0.15-0.36%),而参考队列为 0.46%(86/18546)(95%CI 0.37-0.56%)。致敏的风险比(RR)为 0.55(95%CI 0.35-0.87),且具有统计学意义(p=0.009)。绝对风险差异为 0.20%,相当于需要治疗的人数(NNT)为 500。
在第一孕期使用非侵入性产前筛查胎儿 RHD,选择性地针对携带 RHD 阳性胎儿的 RHD 阴性孕妇进行常规产前抗-D 预防,可显著降低新的 RhD 免疫发生率。这种风险降低与评估非选择性 RAADP 对所有 RHD 阴性妇女的结果的研究报告的风险降低相当。这种有针对性方法的成本效益仍有待研究。