Bhaskar Atul, Patni Piyush
Children Orthopaedic Clinic, Apt 003/18, MHADA Complex, Off Link Road, Nr Maheshwari Bhavan, Oshiwara, Andheri West, Mumbai, India.
Indian J Orthop. 2013 Jul;47(4):370-6. doi: 10.4103/0019-5413.114921.
Relapse of clubfoot deformity following correction by Ponseti technique is not uncommon. The relapsed feet progress from flexible to rigid if left untreated and can become as severe as the initial deformity. No definitive classification exists to assess a relapsed clubfoot. Some authors have used the Pirani score to rate the relapse while others have used descriptive terms. The purpose of this study is to analyze the relapse pattern in clubfeet that have undergone treatment with the Ponseti method and propose a simple classification for relapsed clubfeet.
Ninety-one children (164 feet) with idiopathic clubfeet who underwent treatment with Ponseti technique presented with relapse of the deformity. There were 68 boys and 23 girls. Mean age at presentation for casting was 10.71 days (range 7-22 days). Seventy three children (146 feet, 80%) had bilateral involvement and 18 (20%) had unilateral clubfeet. The mean Pirani Score was 5.6 and 5.5 in bilateral and unilateral groups respectively. Percutaneous heel cord tenotomy was done in 65 children (130 feet, 89%) in the bilateral group and in 12 children (66%) with unilateral clubfoot.
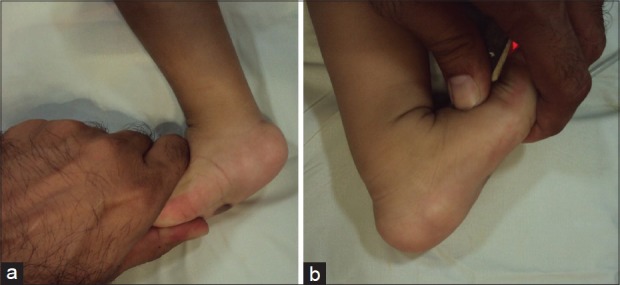
Five relapse patterns were identified at a mean followup of 4.5 years (range 3-5 years) which forms the basis of this study. These relapse patterns were classified as: Grade IA: decrease in ankle dorsiflexion from15 degrees to neutral, Grade IB: dynamic forefoot adduction or supination, Grade IIA - rigid equinus, Grade IIB - rigid adduction of forefoot/midfoot complex and Grade III: combination of two or more deformities: Fixed equinus, varus and forefoot adduction. In the bilateral group, 21 children (38 feet, 28%) had Grade IA relapse. Twenty four children (46 feet, 34%) had dynamic intoeing (Grade IB) on walking. Thirteen children (22 feet, 16%) had true ankle equinus of varying degress (Grade IIA); eight children (13 feet, 9.7%) had fixed adduction deformity of the forefoot (Grade IIB) and seven children (14 feet, 10.7%) had two or more fixed deformities. In the unilateral group seven cases (38%) had reduced dorsiflexion (Grade IA), six (33%) had dynamic adduction (Grade IB), two (11%) had fixed equinus and adduction respectively (Grade IIA and IIB) and one (5%) child had fixed equinus and adduction deformity (Grade III). The relapses were treated by full time splint application, re-casting, tibialis anterior transfer, posterior release, corrective lateral closing wedge osteotomy and a comprehensive subtalar release. Splint compliance was compromised in both groups.
Relapse pattern in clubfeet can be broadly classified into three distinct subsets. Early identification of relapses and early intervention will prevent major soft tissue surgery. A universal language of relapse pattern will allow comparison of results of intervention.
经庞塞蒂(Ponseti)技术矫正后马蹄内翻足畸形复发并不罕见。如果不进行治疗,复发的足部会从柔软畸形发展为僵硬畸形,严重程度可能与初始畸形相同。目前尚无用于评估复发马蹄内翻足的明确分类方法。一些作者使用皮拉尼(Pirani)评分来评估复发情况,而其他作者则使用描述性术语。本研究的目的是分析接受庞塞蒂方法治疗的马蹄内翻足的复发模式,并为复发的马蹄内翻足提出一种简单的分类方法。
91例(164足)特发性马蹄内翻足患儿接受庞塞蒂技术治疗后出现畸形复发。其中男孩68例,女孩23例。初次石膏固定时的平均年龄为10.71天(范围7 - 22天)。73例患儿(146足,80%)为双侧受累,18例(20%)为单侧马蹄内翻足。双侧组和单侧组的平均皮拉尼评分别为5.6和5.5。双侧组65例患儿(130足,89%)及单侧马蹄内翻足患儿中的12例(66%)接受了经皮跟腱切断术。
在平均4.5年(范围3 - 5年)的随访中确定了五种复发模式,这构成了本研究的基础。这些复发模式分类如下:IA级:踝关节背屈从15度降至中立位;IB级:动态性前足内收或旋后;IIA级 - 僵硬性马蹄足;IIB级 - 前足/中足复合体僵硬性内收;III级:两种或更多畸形的组合:固定性马蹄足、内翻足和前足内收。在双侧组中,21例患儿(38足,28%)出现IA级复发。24例患儿(46足,34%)行走时出现动态性内旋(IB级)。13例患儿(22足,16%)有不同程度的真性踝关节马蹄足(IIA级);8例患儿(13足,9.7%)有前足固定性内收畸形(IIB级),7例患儿(14足,10.7%)有两种或更多固定性畸形。在单侧组中,7例(38%)出现背屈减少(IA级),6例(33%)出现动态性内收(IB级),2例(11%)分别出现固定性马蹄足和内收(IIA级和IIB级),1例(5%)患儿有固定性马蹄足和内收畸形(III级)。复发采用全天佩戴支具、重新石膏固定、胫前肌移位、后路松解、矫正性外侧闭合楔形截骨术和综合性距下关节松解术进行治疗。两组中支具佩戴依从性均较差。
马蹄内翻足的复发模式可大致分为三个不同的亚组。早期识别复发并早期干预可避免进行大型软组织手术。复发模式的通用语言将有助于比较干预结果。


