Lao Christopher D, Friedman Judah, Tsien Christina I, Normolle Daniel P, Chapman Christopher, Cao Yue, Lee Oliver, Schipper Matt, Van Poznak Catherine, Hamstra Daniel, Lawrence Theodore, Hayman James, Redman Bruce G
Radiat Oncol. 2013 Aug 21;8:204. doi: 10.1186/1748-717X-8-204.
Survival of patients with brain metastasis particularly from historically more radio-resistant malignancies remains dismal. A phase I study of concurrent bortezomib and whole brain radiotherapy was conducted to determine the tolerance and safety of this approach in patients with previously untreated brain metastasis.
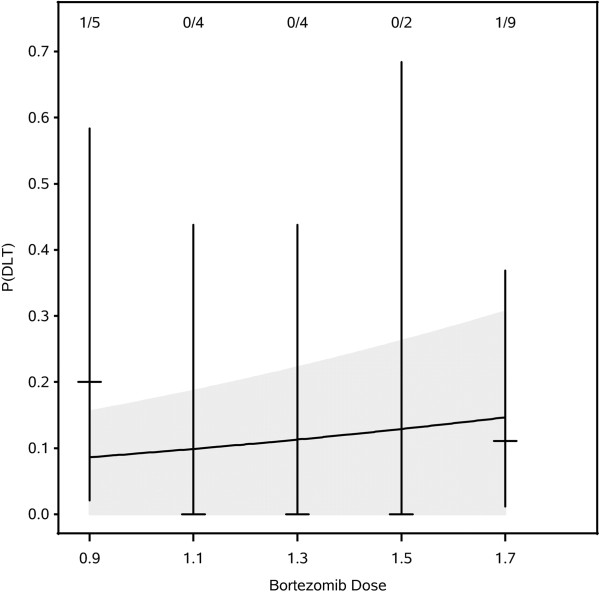
A phase I dose escalation study evaluated the safety of bortezomib (0.9, 1.1, 1.3, 1.5, and 1.7 mg/m2) given on days 1, 4, 8 and 11 of whole brain radiotherapy. Patients with confirmed brain metastasis were recruited for participation. The primary endpoint was the dose-limiting toxicity, defined as any ≥ grade 3 non-hematologic toxicity or grade ≥ 4 hematologic toxicity from the start of treatment to one month post irradiation. Time-to-Event Continual Reassessment Method (TITE-CRM) was used to determine dose escalation. A companion study of brain diffusion tensor imaging MRI was conducted on a subset of patients to assess changes in the brain that might predict delayed cognitive effects.
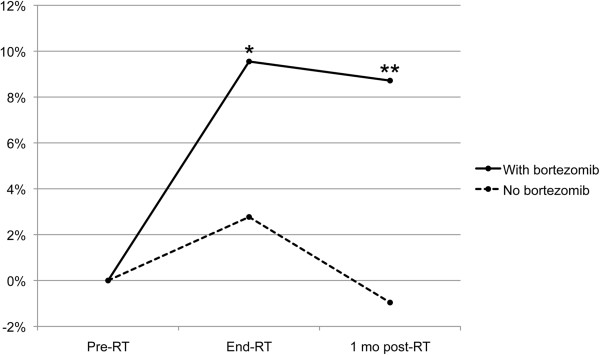
Twenty-four patients were recruited and completed the planned therapy. Patients with melanoma accounted for 83% of all participants. The bortezomib dose was escalated as planned to the highest dose of 1.7 mg/m2/dose. No grade 4/5 toxicities related to treatment were observed. Two patients had grade 3 dose-limiting toxicities (hyponatremia and encephalopathy). A partial or minor response was observed in 38% of patients. Bortezomib showed greater demyelination in hippocampus-associated white matter structures on MRI one month after radiotherapy compared to patients not treated with bortezomib (increase in radial diffusivity +16.8% versus 4.8%; p = 0.0023).
Concurrent bortezomib and whole brain irradiation for brain metastasis is well tolerated at one month follow-up, but MRI changes that have been shown to predict delayed cognitive function can be detected within one month of treatment.
脑转移患者,尤其是那些来自既往对放疗更具抗性的恶性肿瘤患者,其生存率仍然很低。开展了一项硼替佐米与全脑放疗联合应用的I期研究,以确定该方法在既往未经治疗的脑转移患者中的耐受性和安全性。
一项I期剂量递增研究评估了在全脑放疗的第1、4、8和11天给予硼替佐米(0.9、1.1、1.3、1.5和1.7mg/m²)的安全性。招募确诊为脑转移的患者参与研究。主要终点是剂量限制毒性,定义为从治疗开始至放疗后1个月内出现的任何≥3级非血液学毒性或≥4级血液学毒性。采用事件发生时间连续重新评估法(TITE-CRM)来确定剂量递增。对一部分患者进行了脑扩散张量成像MRI的配套研究,以评估可能预测延迟认知效应的脑部变化。
招募了24名患者并完成了计划治疗。黑色素瘤患者占所有参与者的83%。硼替佐米剂量按计划递增至最高剂量1.7mg/m²/剂量。未观察到与治疗相关的4/5级毒性。2名患者出现3级剂量限制毒性(低钠血症和脑病)。38%的患者观察到部分缓解或轻微缓解。与未接受硼替佐米治疗的患者相比,放疗后1个月时,接受硼替佐米治疗的患者在MRI上显示海马相关白质结构的脱髓鞘更明显(径向扩散率增加16.8%对4.8%;p=0.0023)。
在随访1个月时,硼替佐米与全脑照射联合用于脑转移的耐受性良好,但在治疗1个月内即可检测到已被证明可预测延迟认知功能的MRI变化。