Department of Pharmacy, National Center for Geriatrics and Gerontology, Obu, Aichi, Japan.
Clin Interv Aging. 2013;8:1015-21. doi: 10.2147/CIA.S50238. Epub 2013 Aug 7.
Methicillin-resistant Staphylococcus aureus (MRSA) infections are associated with significant mortality and health care costs. To improve treatment outcomes for MRSA, a better understanding of the pharmacokinetic/pharmacodynamic parameters of vancomycin is required to develop optimal dosing strategies, particularly in elderly patients (≥75 years of age) with limited renal function. The purpose of this study was to determine whether pharmacokinetic indices for vancomycin are associated with mortality from MRSA hospital-acquired pneumonia in elderly patients.
We conducted a retrospective observational study with 28-day mortality as the primary outcome for 94 patients with MRSA hospital-acquired pneumonia who had been treated with vancomycin from January 2006 through December 2012. Our most recent sampling of MRSA isolates had a minimum inhibitory concentration (MIC) for vancomycin of 1 μg/mL (86%), indicating that the area under the curve (AUC) was equal to the AUC/MIC in these isolates. The primary data from 28-day survivors and nonsurvivors were compared.
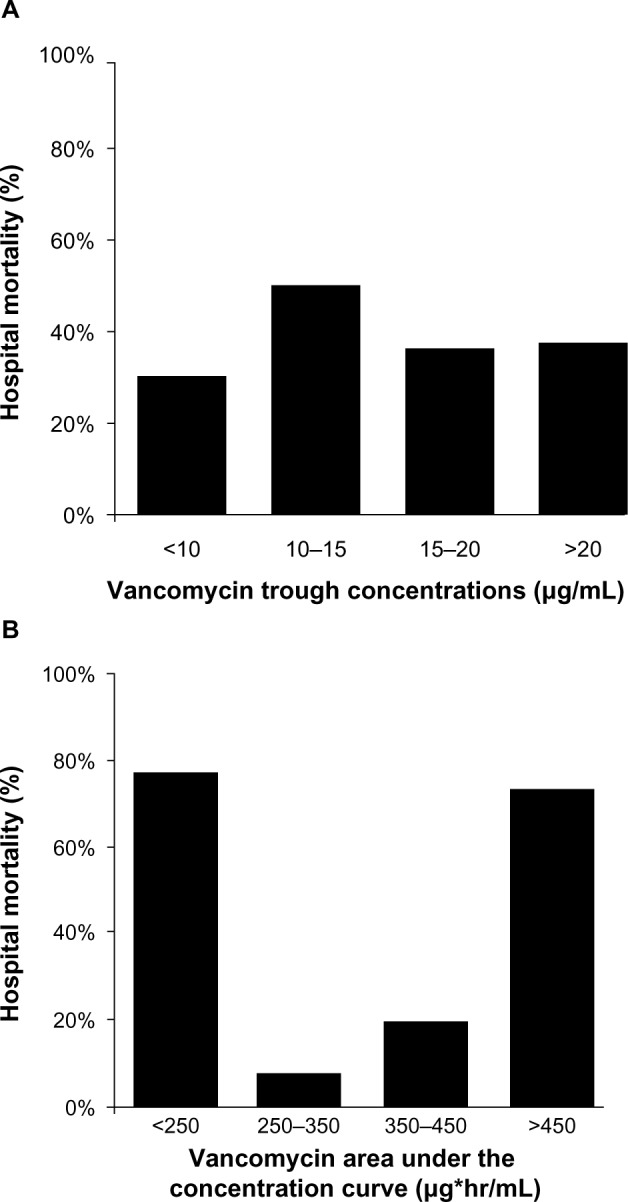
Among 94 elderly patients, the mean age was 82 (75-99) years. Multivariate analyses revealed that, among the factors examined, only the nonoptimal AUC (<250, >450 μg*h/mL) was an independent predictor of 28-day mortality in elderly patients (odds ratio 23.156, 95% confidence interval 6.814-78.687, P < 0.001). We detected a significant difference for increasing nephrotoxicity in nonsurvivors (nine of 32 patients [28%]) compared with survivors (three of 62 patients [4.8%], P = 0.003).
This finding indicates that patients with potentially poor renal function are likely to have increased AUC values and a poor prognosis. Consideration of the pharmacokinetics/pharmacodynamics of vancomycin and targeting an AUC/MIC value of 250-450 μg*h/mL may result in improved treatment outcomes for elderly patients with MRSA hospital-acquired pneumonia.
耐甲氧西林金黄色葡萄球菌(MRSA)感染与显著的死亡率和医疗保健费用相关。为了改善 MRSA 的治疗结果,需要更好地了解万古霉素的药代动力学/药效动力学参数,以制定最佳的给药策略,特别是在肾功能有限的老年患者(≥75 岁)中。本研究的目的是确定万古霉素的药代动力学指标是否与老年患者 MRSA 医院获得性肺炎的死亡率相关。
我们进行了一项回顾性观察研究,以 28 天死亡率为主要结局,纳入了 94 例 2006 年 1 月至 2012 年 12 月期间接受万古霉素治疗的 MRSA 医院获得性肺炎患者。我们最近对 MRSA 分离株的最小抑菌浓度(MIC)进行了采样,万古霉素的 MIC 为 1μg/ml(86%),这表明这些分离株的 AUC 等于 AUC/MIC。比较了 28 天幸存者和非幸存者的主要数据。
在 94 名老年患者中,平均年龄为 82(75-99)岁。多变量分析显示,在所检查的因素中,只有非最佳 AUC(<250,>450μg*h/ml)是老年患者 28 天死亡率的独立预测因素(比值比 23.156,95%置信区间 6.814-78.687,P<0.001)。我们发现,与幸存者(62 例中的 3 例[4.8%])相比,非幸存者的肾毒性增加(32 例中的 9 例[28%])有显著差异(P=0.003)。
这一发现表明,肾功能可能较差的患者可能会有更高的 AUC 值和较差的预后。考虑万古霉素的药代动力学/药效动力学,并将 AUC/MIC 值目标设定为 250-450μg*h/ml,可能会改善老年 MRSA 医院获得性肺炎患者的治疗结果。