Department of Gynecology and Obstetrics, West German Cancer Center, University Clinic Essen, University of Duisburg-Essen, Hufelandstrasse 55, Essen 45147, Germany.
World J Surg Oncol. 2013 Aug 26;11:211. doi: 10.1186/1477-7819-11-211.
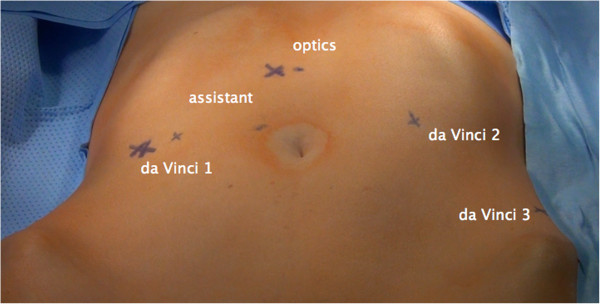
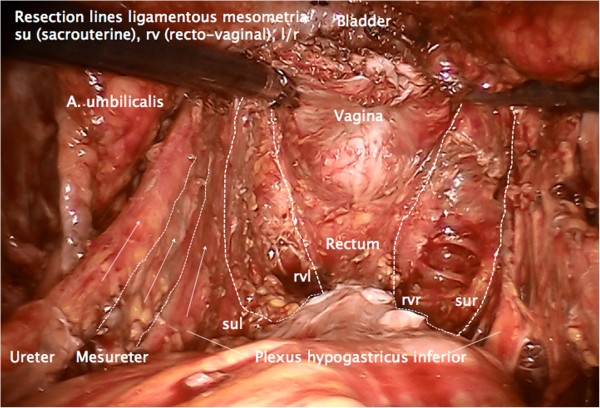
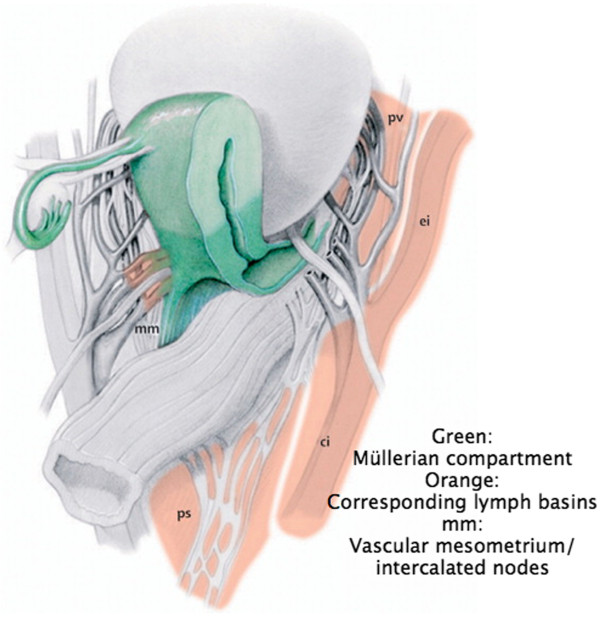
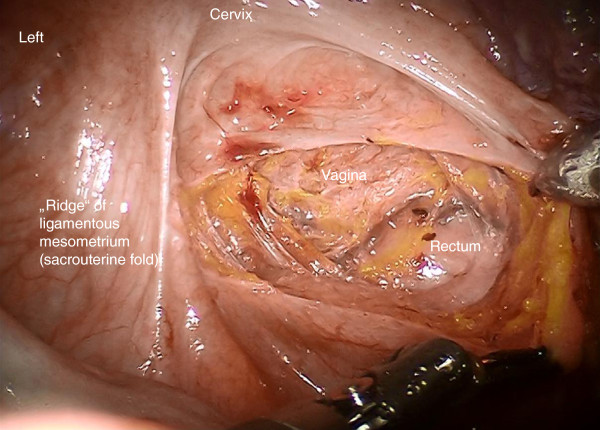
Radical hysterectomy has been developed as a standard treatment in Stage I and II cervical cancers with and without adjuvant therapy. However, there have been several attempts to standardize the technique of radical hysterectomy required for different tumor extension with variable success. Total mesometrial resection as ontogenetic compartment-based oncologic surgery - developed by open surgery - can be standardized identically for all patients with locally defined tumors. It appears to be promising for patients in terms of radicalness as well as complication rates. Robotic surgery may additionally reduce morbidity compared to open surgery. We describe robotically assisted total mesometrial resection (rTMMR) step by step in cervical cancer and present feasibility data from 26 patients.
Patients (n = 26) with the diagnosis of cervical cancer were included. Patients were treated by robotic total mesometrial resection (rTMMR) and pelvic or pelvic/periaortic robotic therapeutic lymphadenectomy (rtLNE) for FIGO stage IA-IIB cervical cancer.
No transition to open surgery was necessary. No intraoperative complications were noted. The postoperative complication rate was 23%. Within follow-up time (mean: 18 months) we noted one distant but no locoregional recurrence of cervical cancer. There were no deaths from cervical cancer during the observation period.
We conclude that rTMMR and rtLNE is a feasible and safe technique for the treatment of compartment-defined cervical cancer.
根治性子宫切除术已发展成为有或无辅助治疗的 I 期和 II 期宫颈癌的标准治疗方法。然而,已经有几次尝试通过不同的成功来规范不同肿瘤扩展所需的根治性子宫切除术技术。全子宫系膜切除术作为基于个体发生隔间的肿瘤学手术-由开放手术发展而来-可以为所有局部定义肿瘤的患者标准化。就根治性和并发症发生率而言,它似乎对患者很有前途。与开放手术相比,机器人手术可能会降低发病率。我们一步一步地描述了宫颈癌的机器人辅助全子宫系膜切除术(rTMMR),并介绍了 26 例患者的可行性数据。
纳入诊断为宫颈癌的患者。对 FIGO 分期为 IA-IIB 期的宫颈癌患者采用机器人全子宫系膜切除术(rTMMR)和盆腔或盆腔/主动脉旁机器人治疗性淋巴结切除术(rtLNE)进行治疗。
无需转为开放手术。未发生术中并发症。术后并发症发生率为 23%。在随访期间(平均 18 个月),我们注意到远处有 1 例宫颈癌复发,但无局部复发。在观察期间无宫颈癌死亡。
我们得出结论,rTMMR 和 rtLNE 是治疗限定在隔间的宫颈癌的一种可行且安全的技术。