Clinical Epidemiology and Outcomes Program, Houston VA Health Services Research and Development Center of Excellence, Houston, Texas; Department of Medicine, Baylor College of Medicine, Houston, Texas; Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas.
Clinical Epidemiology and Outcomes Program, Houston VA Health Services Research and Development Center of Excellence, Houston, Texas; Department of Medicine, Baylor College of Medicine, Houston, Texas.
Clin Gastroenterol Hepatol. 2014 Feb;12(2):327-333.e1. doi: 10.1016/j.cgh.2013.08.034. Epub 2013 Aug 23.
BACKGROUND & AIMS: Interleukin (IL)-28B (interferon-λ 3) genotype is the strongest predictor of response of patients with hepatitis C virus (HCV) infection to antiviral therapy. However, patients with HCV infection often have physical or mental comorbidities that contraindicate or complicate treatment, regardless of their genotype. The potential role of IL28B genotype within the context of patients' clinical and social environment is therefore unclear.
We characterized the IL28B genotype (for rs12980275 and rs8099917) in 308 patients (mean age, 56 y; 25% African American; 38% with advanced-stage fibrosis) with genotype 1 HCV infection seen at the Michael E. DeBakey Veterans Administration Medical Center in Houston, Texas, from May 1, 2009, through April 1, 2012. We evaluated their eligibility for antiviral treatment based on clinical and social factors such as physical or mental health comorbidity, ongoing alcohol or drug use, and noncompliance with treatment evaluation.
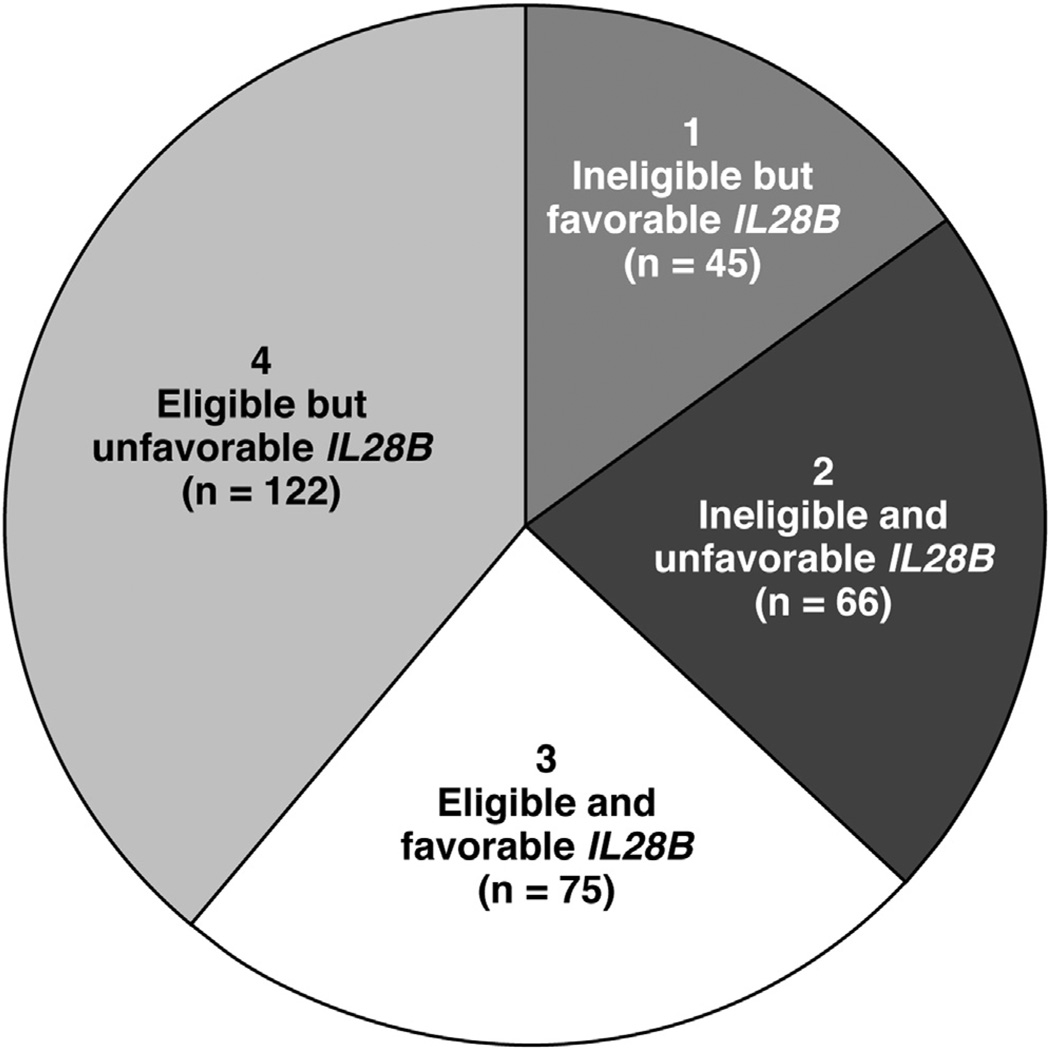
Of the 308 subjects, 40% were homozygous for rs12980275 (associated with response to therapy), 46% were heterozygous, and 15% were homozygous for alleles associated with reduced response to therapy. Overall, 36% of patients were considered to be ineligible for treatment; of these, 40% had the rs12980275 genotype. More than half of the patients with rs12980275 who were ineligible for treatment were excluded because of mental health comorbidities; one-third of these patients had advanced fibrosis. The reason(s) for treatment exclusion resolved in only 8% of patients during a mean 1.5 years of follow-up evaluation.
In a well-characterized cohort of patients with HCV, a large proportion (40%) with IL28B polymorphisms associated with response to therapy is ineligible for treatment because of contraindications. One potential role of IL28B genotype analysis could be to identify patients who, although not currently eligible for antiviral treatment, could become so by modifying fixable exclusions to treatment.
白细胞介素 28B(干扰素-λ3,IL-28B)基因型是丙型肝炎病毒(HCV)感染者对抗病毒治疗反应的最强预测因子。然而,HCV 感染患者常常存在身体或精神合并症,这些合并症会导致治疗受到禁忌或复杂化,而与基因型无关。因此,IL-28B 基因型在患者临床和社会环境中的潜在作用尚不清楚。
我们在 2009 年 5 月 1 日至 2012 年 4 月 1 日期间,在德克萨斯州休斯顿迈克尔 E. 德贝基退伍军人管理医疗中心(Michael E. DeBakey Veterans Administration Medical Center)观察了 308 例基因型 1 HCV 感染患者(平均年龄 56 岁;25%为非裔美国人;38%为晚期纤维化)的 IL28B 基因型(rs12980275 和 rs8099917),并评估了他们基于身体或精神健康合并症、持续饮酒或药物使用以及不遵守治疗评估等临床和社会因素的抗病毒治疗资格。
在 308 名受试者中,40%为 rs12980275 纯合子(与治疗反应相关),46%为杂合子,15%为与治疗反应降低相关的等位基因纯合子。总体而言,36%的患者被认为不适合治疗;其中 40%的患者为 rs12980275 基因型。不适合治疗的 rs12980275 患者中,超过一半的人因精神健康合并症而被排除在外;其中三分之一的患者有晚期纤维化。在平均 1.5 年的随访评估期间,只有 8%的患者在 rs12980275 治疗排除原因得到解决。
在一组特征明确的 HCV 患者中,由于禁忌,与治疗反应相关的 IL28B 多态性的很大一部分(40%)不适合治疗。IL-28B 基因型分析的一个潜在作用可能是确定那些尽管目前不适合抗病毒治疗,但通过修改可纠正的治疗排除因素,将来可能适合治疗的患者。