HIV Epidemiology and Outcomes Research Unit, Section of Infectious Diseases, Boston Medical Center, Boston, Massachusetts, United States of America; Department of Epidemiology, Boston University School of Public Health, Boston, Massachusetts, United States of America.
HIV Epidemiology and Outcomes Research Unit, Section of Infectious Diseases, Boston Medical Center, Boston, Massachusetts, United States of America.
PLoS One. 2014 May 19;9(5):e97317. doi: 10.1371/journal.pone.0097317. eCollection 2014.
As highly effective hepatitis C virus (HCV) therapies emerge, data are needed to inform the development of interventions to improve HCV treatment rates. We used simulation modeling to estimate the impact of loss to follow-up on HCV treatment outcomes and to identify intervention strategies likely to provide good value for the resources invested in them.
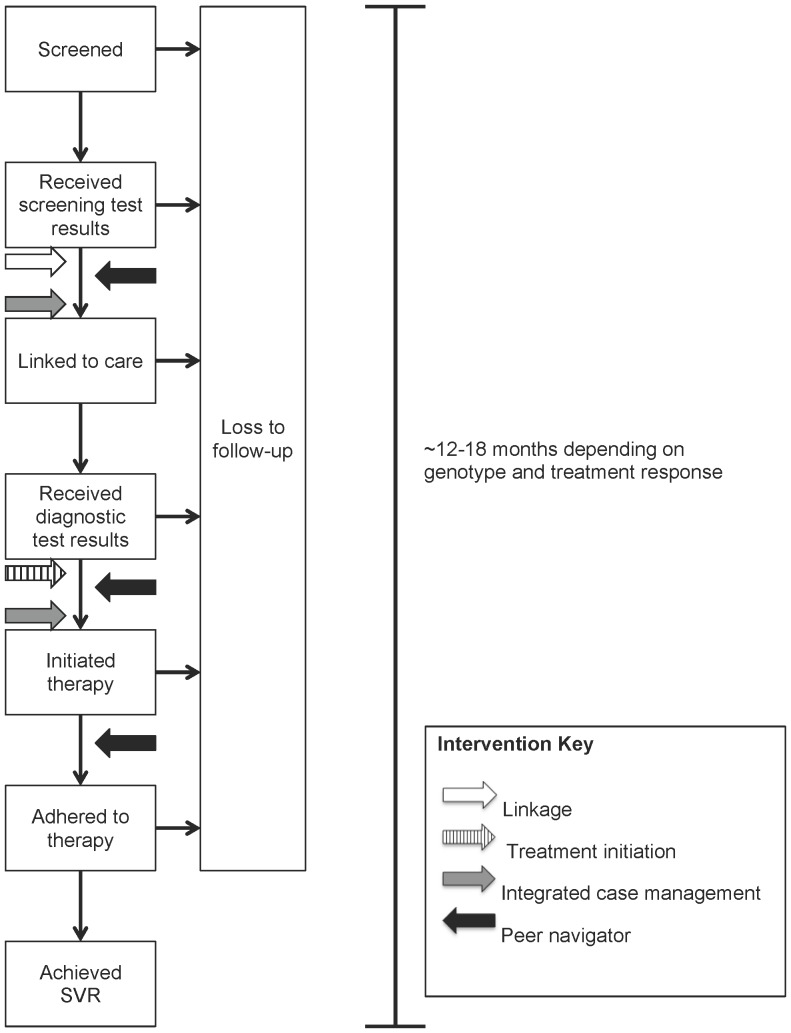
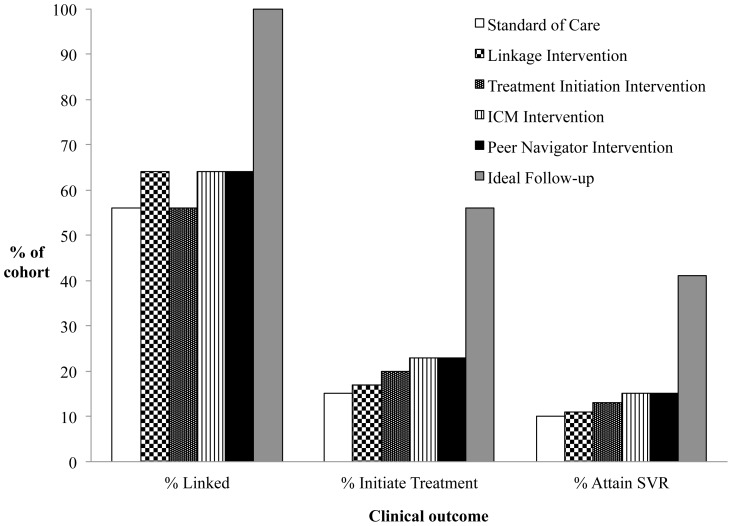
We used a Monte Carlo state-transition model to simulate a hypothetical cohort of chronically HCV-infected individuals recently screened positive for serum HCV antibody. We simulated four hypothetical intervention strategies (linkage to care; treatment initiation; integrated case management; peer navigator) to improve HCV treatment rates, varying efficacies and costs, and identified strategies that would most likely result in the best value for the resources required for implementation.
Sustained virologic responses (SVRs), life expectancy, quality-adjusted life expectancy (QALE), costs from health system and program implementation perspectives, and incremental cost-effectiveness ratios (ICERs).
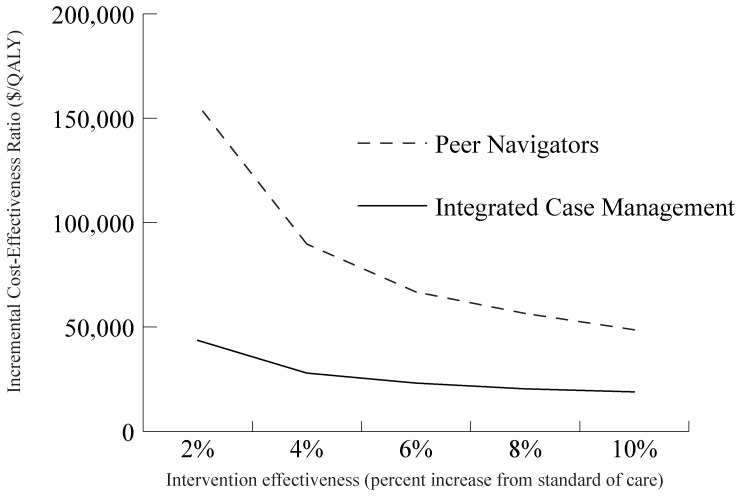
We estimate that imperfect follow-up reduces the real-world effectiveness of HCV therapies by approximately 75%. In the base case, a modestly effective hypothetical peer navigator program maximized the number of SVRs and QALE, with an ICER compared to the next best intervention of $48,700/quality-adjusted life year. Hypothetical interventions that simultaneously addressed multiple points along the cascade provided better outcomes and more value for money than less costly interventions targeting single steps. The 5-year program cost of the hypothetical peer navigator intervention was $14.5 million per 10,000 newly diagnosed individuals.
We estimate that imperfect follow-up during the HCV cascade of care greatly reduces the real-world effectiveness of HCV therapy. Our mathematical model shows that modestly effective interventions to improve follow-up would likely be cost-effective. Priority should be given to developing and evaluating interventions addressing multiple points along the cascade rather than options focusing solely on single points.
随着高效的丙型肝炎病毒 (HCV) 治疗方法的出现,需要数据来为提高 HCV 治疗率的干预措施提供信息。我们使用模拟模型来估计失访对 HCV 治疗结果的影响,并确定可能为投资资源提供良好价值的干预策略。
我们使用蒙特卡罗状态转移模型来模拟一组最近 HCV 抗体血清筛查阳性的慢性 HCV 感染个体的假设队列。我们模拟了四种假设的干预策略(链接至护理;治疗启动;综合病例管理;同伴导航员)来提高 HCV 治疗率,改变疗效和成本,并确定最有可能为实施所需资源提供最佳价值的策略。
持续病毒学应答 (SVR)、预期寿命、质量调整生命期望 (QALE)、从卫生系统和方案实施角度来看的成本以及增量成本效益比 (ICER)。
我们估计,不完美的随访会使 HCV 治疗的实际效果降低约 75%。在基础情况下,一个适度有效的假设同伴导航员计划最大限度地提高了 SVR 和 QALE 的数量,与下一个最佳干预措施相比,ICER 为 48700 美元/质量调整生命年。与针对单一步骤的成本较低的干预措施相比,同时针对级联中多个点的假设干预措施提供了更好的结果和更高的性价比。假设同伴导航员干预计划的 5 年方案成本为每 10000 名新诊断个体 1450 万美元。
我们估计,在 HCV 护理级联中不完美的随访大大降低了 HCV 治疗的实际效果。我们的数学模型表明,改善随访的适度有效的干预措施可能具有成本效益。应优先考虑开发和评估针对级联中多个点的干预措施,而不是仅关注单一点的方案。