Department of Clinical Immunology, Hôpital Saint-Louis, Assistance Publique-Hôpitaux de Paris, Paris, France; Univ Paris Diderot, Sorbonne Paris Cité, Paris, France.
Eur J Haematol. 2013 Dec;91(6):497-503. doi: 10.1111/ejh.12191. Epub 2013 Sep 18.
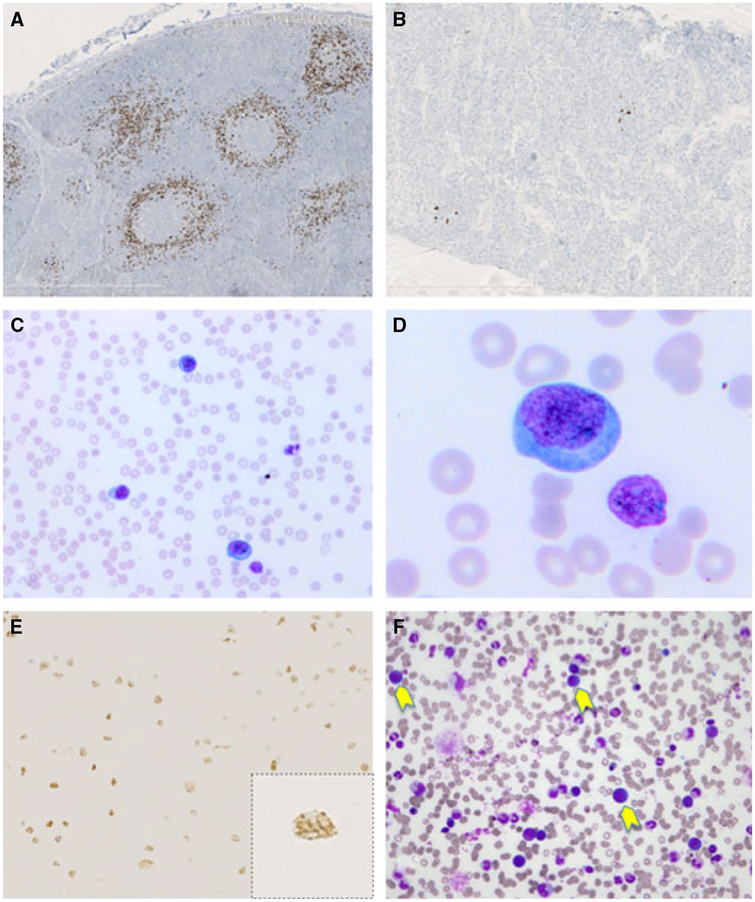
Multicentric Castleman disease (MCD) is a distinct lymphoproliferative disorder characterized by inflammatory symptoms, lymphadenopathy, splenomegaly, and cytopenia. Kaposi's sarcoma-associated herpesvirus (KSHV), also called human herpesvirus-8 (HHV-8), is the cause of virtually all cases of MCD occurring in patients with HIV infection. MCD lesions characteristically contain HHV-8-infected polyclonal IgMλ plasmablasts. A high frequency of HHV-8-related non-Hodgkin lymphoma has been reported in these patients.
We now report on three patients who presented with severe symptoms of MCD, extreme splenomegaly, and rapid expansion of B-cell lymphocytosis (44-81%) attributable to circulating HHV-8 positive plasmablasts.
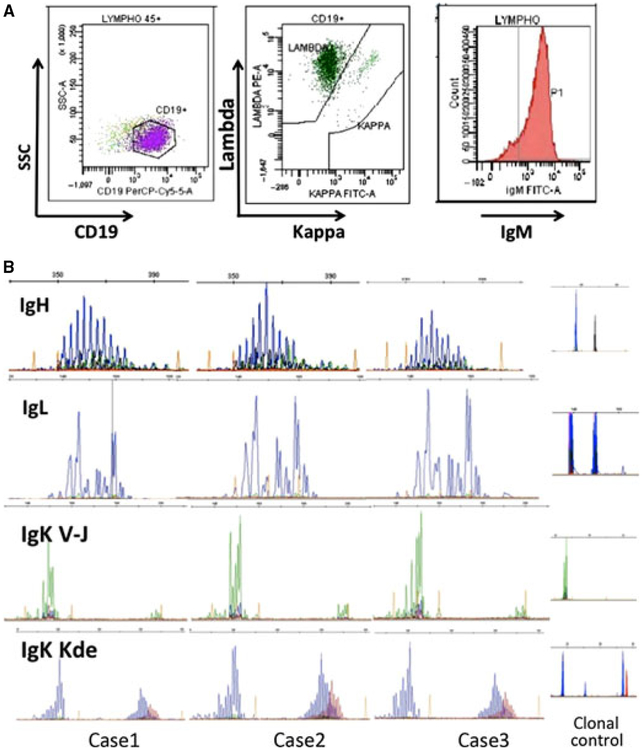
The circulating plasmablastic cells shared the phenotype (IgMλ, CD19+, CD20- CD138-) of HHV-8-infected cells from MCD lesions, mimicking the leukemic phase of large B-cell lymphoma occurring in HHV-8-related MCD. These patients displayed a very high HHV-8 viral load in blood (>7 logs HHV-8 DNA copies/ml) and high levels of serum vIL-6, the viral homolog of human interleukin 6. Serum IL-6 and IL-10 were also abnormally elevated. HHV-8-infected cells were demonstrated by immunoglobulin gene rearrangement analysis, to be polyclonal and likely represent an expansion of HHV-8-infected cells similar to those found in MCD lesions.
Thus, the spectrum of HHV-8-related plasmablastic lymphoproliferative disorders in patients with HIV infection is expanded to include HHV-8+ polyclonal IgMλ B-cell lymphocytosis. At onset, this lymphoproliferative disorder may mimic plasmablastic leukemia/lymphoma. Recognizing this unusual complication may have important implications in treatment decision avoiding unnecessary toxicity to the patients.
多中心卡斯特曼病(MCD)是一种独特的淋巴增生性疾病,其特征为炎症症状、淋巴结病、脾肿大和细胞减少症。卡波西肉瘤相关疱疹病毒(KSHV),也称为人类疱疹病毒 8(HHV-8),是几乎所有发生在 HIV 感染患者中的 MCD 的病因。MCD 病变特征性地包含 HHV-8 感染的多克隆 IgMλ 浆母细胞。这些患者中已报道有很高的 HHV-8 相关非霍奇金淋巴瘤的发病率。
我们现在报告三例患者,他们表现出严重的 MCD 症状、极度脾肿大和 B 细胞淋巴增生(44-81%)的快速扩张,归因于循环的 HHV-8 阳性浆母细胞。
循环浆母细胞具有与 MCD 病变中 HHV-8 感染细胞相同的表型(IgMλ、CD19+、CD20-CD138-),模拟了发生在 HHV-8 相关 MCD 中的大 B 细胞淋巴瘤的白血病期。这些患者的血液中 HHV-8 病毒载量非常高(>7 对数 HHV-8 DNA 拷贝/ml),血清 vIL-6(病毒人白细胞介素 6 的同系物)水平也很高。血清 IL-6 和 IL-10 也异常升高。通过免疫球蛋白基因重排分析证明 HHV-8 感染细胞是多克隆的,可能代表与 MCD 病变中发现的相似的 HHV-8 感染细胞的扩增。
因此,在 HIV 感染患者中,HHV-8 相关浆母细胞性淋巴增生性疾病的谱扩大到包括 HHV-8+多克隆 IgMλ B 细胞淋巴增生。在发病时,这种淋巴增生性疾病可能模拟浆母细胞白血病/淋巴瘤。认识到这种不寻常的并发症可能对治疗决策有重要影响,避免对患者产生不必要的毒性。