Cardiovascular Division, Brigham and Women's Hospital, Boston, Massachusetts; Division of Cardiology, Department of Medicine, Massachusetts General Hospital, Boston, Massachusetts; Cardiac MR PET CT Program, Department of Radiology, Massachusetts General Hospital, Boston, Massachusetts.
J Am Coll Cardiol. 2013 Dec 10;62(23):2205-14. doi: 10.1016/j.jacc.2013.07.067. Epub 2013 Aug 28.
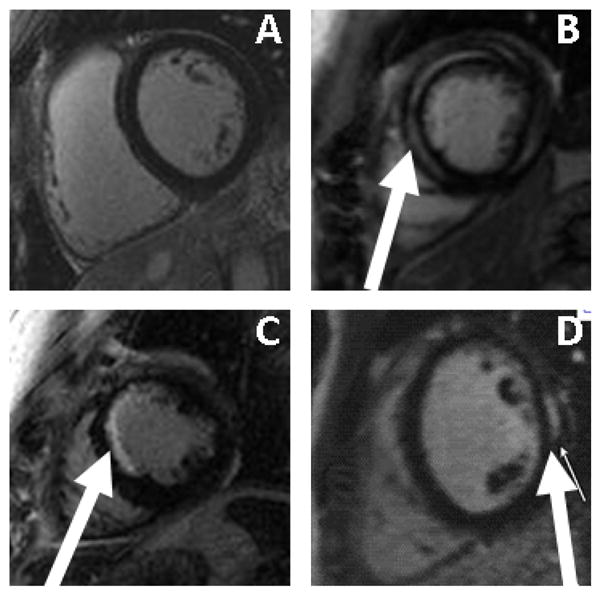
This study sought to identify the frequency, pattern, and prognostic significance of left ventricular (LV) late gadolinium enhancement (LGE) in patients with atrial fibrillation (AF).
There are limited data on the presence, pattern, and prognostic significance of LV myocardial fibrosis in patients with AF. LGE during cardiac magnetic resonance imaging is a marker for myocardial fibrosis.
A group of 664 consecutive patients without known prior myocardial infarction who were referred for radiofrequency ablation of AF were studied. Cardiac magnetic resonance imaging was requested to assess pulmonary venous anatomy.
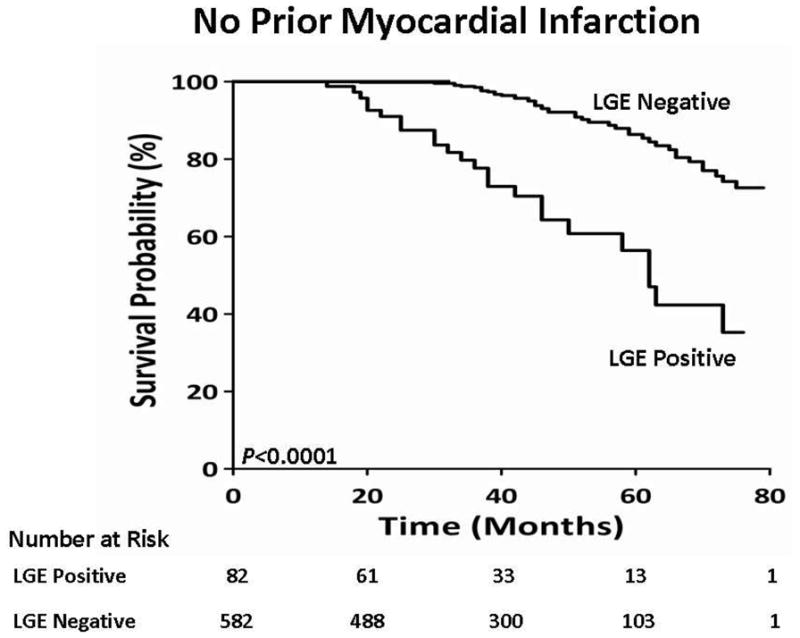
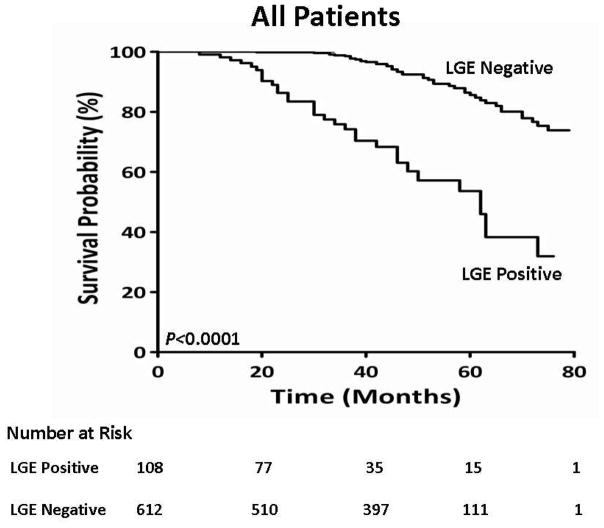
Overall, 73% were men, with a mean age of 56 years and a mean LV ejection fraction of 56 ± 10%. LV LGE was found in 88 patients (13%). The endpoint was all-cause mortality, and in this cohort, 68 deaths were observed over a median follow-up period of 42 months. On univariate analysis, age (hazard ratio [HR]: 1.05; 95% confidence interval [CI]: 1.03 to 1.08; chi-square likelihood ratio [LRχ(2)]: 15.2; p = 0.0001), diabetes (HR: 2.39; 95% CI: 1.41 to 4.09; LRχ(2): 10.3; p = 0.001), a history of heart failure (HR: 1.78; 95% CI: 1.09 to 2.91; LRχ(2): 5.37; p = 0.02), left atrial dimension (HR: 1.04; 95% CI: 1.01 to 1.08; LRχ(2): 6.47; p = 0.01), presence of LGE (HR: 5.08; 95% CI: 3.08 to 8.36; LRχ(2): 28.8; p < 0.0001), and LGE extent (HR: 1.15; 95% CI: 1.10 to 1.21; LRχ(2): 35.6; p < 0.0001) provided the strongest associations with mortality. The mortality rate was 8.1% per patient-year in patients with LGE compared with 2.3% patients without LGE. In the best overall multivariate model for mortality, age and the extent of LGE were independent predictors of mortality. Indeed, each 1% increase in the extent of LGE was associated with a 15% increased risk for death.
In patients with AF, LV LGE is a frequent finding and is a powerful predictor of mortality.
本研究旨在确定心房颤动(AF)患者左心室(LV)晚期钆增强(LGE)的频率、模式和预后意义。
关于 AF 患者 LV 心肌纤维化的存在、模式和预后意义的数据有限。心脏磁共振成像中的 LGE 是心肌纤维化的标志物。
对 664 例连续就诊且无已知先前心肌梗死的 AF 射频消融患者进行研究。要求进行心脏磁共振成像以评估肺静脉解剖结构。
总体而言,73%为男性,平均年龄为 56 岁,平均 LV 射血分数为 56 ± 10%。88 例(13%)患者存在 LV LGE。终点是全因死亡率,在该队列中,中位随访 42 个月期间观察到 68 例死亡。单因素分析显示,年龄(风险比[HR]:1.05;95%置信区间[CI]:1.03 至 1.08;卡方似然比[LRχ²]:15.2;p = 0.0001)、糖尿病(HR:2.39;95%CI:1.41 至 4.09;LRχ²:10.3;p = 0.001)、心力衰竭史(HR:1.78;95%CI:1.09 至 2.91;LRχ²:5.37;p = 0.02)、左心房大小(HR:1.04;95%CI:1.01 至 1.08;LRχ²:6.47;p = 0.01)、LGE 存在(HR:5.08;95%CI:3.08 至 8.36;LRχ²:28.8;p < 0.0001)和 LGE 程度(HR:1.15;95%CI:1.10 至 1.21;LRχ²:35.6;p < 0.0001)与死亡率最强相关。与无 LGE 的患者相比,有 LGE 的患者的死亡率为每年 8.1%。在用于死亡率的最佳综合多变量模型中,年龄和 LGE 程度是死亡率的独立预测因素。实际上,LGE 程度每增加 1%,死亡风险就会增加 15%。
在 AF 患者中,LV LGE 是一种常见的发现,是死亡率的有力预测因子。