Zhang Lili, Awadalla Magid, Mahmood Syed S, Nohria Anju, Hassan Malek Z O, Thuny Franck, Zlotoff Daniel A, Murphy Sean P, Stone James R, Golden Doll Lauren Alexandra, Alvi Raza M, Rokicki Adam, Jones-O'Connor Maeve, Cohen Justine V, Heinzerling Lucie M, Mulligan Connor, Armanious Merna, Barac Ana, Forrestal Brian J, Sullivan Ryan J, Kwong Raymond Y, Yang Eric H, Damrongwatanasuk Rongras, Chen Carol L, Gupta Dipti, Kirchberger Michael C, Moslehi Javid J, Coelho-Filho Otavio R, Ganatra Sarju, Rizvi Muhammad A, Sahni Gagan, Tocchetti Carlo G, Mercurio Valentina, Mahmoudi Michael, Lawrence Donald P, Reynolds Kerry L, Weinsaft Jonathan W, Baksi A John, Ederhy Stephane, Groarke John D, Lyon Alexander R, Fradley Michael G, Thavendiranathan Paaladinesh, Neilan Tomas G
Cardiovascular Imaging Research Center (CIRC), Division of Cardiology, Department of Radiology, Massachusetts General Hospital, 165 Cambridge Street, Suite 400, Boston, MA 02114, USA.
Cardio-Oncology Program, Division of Cardiology, Department of Medicine, Massachusetts General Hospital, 165 Cambridge Street, Suite 400, Boston, MA 02114, USA.
Eur Heart J. 2020 May 7;41(18):1733-1743. doi: 10.1093/eurheartj/ehaa051.
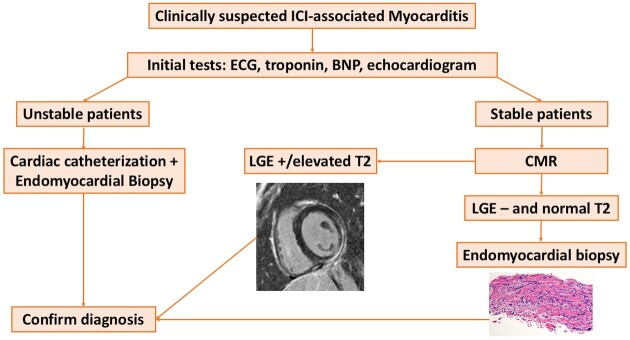
Myocarditis is a potentially fatal complication of immune checkpoint inhibitors (ICI). Sparse data exist on the use of cardiovascular magnetic resonance (CMR) in ICI-associated myocarditis. In this study, the CMR characteristics and the association between CMR features and cardiovascular events among patients with ICI-associated myocarditis are presented.
From an international registry of patients with ICI-associated myocarditis, clinical, CMR, and histopathological findings were collected. Major adverse cardiovascular events (MACE) were a composite of cardiovascular death, cardiogenic shock, cardiac arrest, and complete heart block. In 103 patients diagnosed with ICI-associated myocarditis who had a CMR, the mean left ventricular ejection fraction (LVEF) was 50%, and 61% of patients had an LVEF ≥50%. Late gadolinium enhancement (LGE) was present in 48% overall, 55% of the reduced EF, and 43% of the preserved EF cohort. Elevated T2-weighted short tau inversion recovery (STIR) was present in 28% overall, 30% of the reduced EF, and 26% of the preserved EF cohort. The presence of LGE increased from 21.6%, when CMR was performed within 4 days of admission to 72.0% when CMR was performed on Day 4 of admission or later. Fifty-six patients had cardiac pathology. Late gadolinium enhancement was present in 35% of patients with pathological fibrosis and elevated T2-weighted STIR signal was present in 26% with a lymphocytic infiltration. Forty-one patients (40%) had MACE over a follow-up time of 5 months. The presence of LGE, LGE pattern, or elevated T2-weighted STIR were not associated with MACE.
These data suggest caution in reliance on LGE or a qualitative T2-STIR-only approach for the exclusion of ICI-associated myocarditis.
心肌炎是免疫检查点抑制剂(ICI)的一种潜在致命并发症。关于心血管磁共振(CMR)在ICI相关性心肌炎中的应用数据稀少。本研究呈现了ICI相关性心肌炎患者的CMR特征以及CMR特征与心血管事件之间的关联。
从一个ICI相关性心肌炎患者的国际登记处收集临床、CMR和组织病理学结果。主要不良心血管事件(MACE)包括心血管死亡、心源性休克、心脏骤停和完全性心脏传导阻滞。在103例诊断为ICI相关性心肌炎且接受了CMR检查的患者中,平均左心室射血分数(LVEF)为50%,61%的患者LVEF≥50%。总体上48%的患者存在延迟钆增强(LGE),LVEF降低的患者中55%存在LGE,LVEF保留的患者队列中43%存在LGE。总体上28%的患者T2加权短tau反转恢复(STIR)升高,LVEF降低的患者中30%存在STIR升高,LVEF保留的患者队列中26%存在STIR升高。当在入院后4天内进行CMR检查时,LGE的存在率为21.6%,而在入院第4天或之后进行CMR检查时,LGE的存在率为72.0%。56例患者有心脏病理学检查结果。35%有病理纤维化的患者存在延迟钆增强,26%有淋巴细胞浸润的患者T2加权STIR信号升高。在5个月的随访期内,41例患者(40%)发生了MACE。LGE的存在、LGE模式或T2加权STIR升高与MACE无关。
这些数据提示在仅依靠LGE或定性的仅T2-STIR方法排除ICI相关性心肌炎时需谨慎。