Department of Surgery, Kantonsspital St, Gallen, CH-9007, St, Gallen, Switzerland.
BMC Anesthesiol. 2013 Sep 9;13(1):19. doi: 10.1186/1471-2253-13-19.
Postoperative nausea and vomiting after general anesthesia is not only an unpleasant problem affecting 20-30% of surgical patients but may also lead to severe postoperative complications. There is a particularly high incidence of postoperative nausea and vomiting following thyroidectomy. Dexamethasone has been described as highly effective against chemotherapy-induced nausea and vomiting and has been proposed as a first-line method of postoperative nausea and vomiting prophylaxis. Despite this possible beneficial effect, the prophylactic administration of dexamethasone before surgery to prevent or ameliorate postoperative nausea and vomiting has not been established. A bilateral superficial cervical plexus block during thyroid surgery under general anesthesia significantly reduces pain. Of even greater clinical importance, this block prevents the need for postoperative opioids. Therefore, patients undergoing thyroidectomy and a bilateral superficial cervical plexus block are an ideal group to investigate the efficacy of dexamethasone for postoperative nausea and vomiting. These patients have a high incidence of postoperative nausea and vomiting and do not require opioids. They have no abdominal surgery, which can cause nausea and vomiting via a paralytic ileus. Combined with the highly standardized anesthesia protocol in use at our institution, this setting allows all known biases to be controlled.
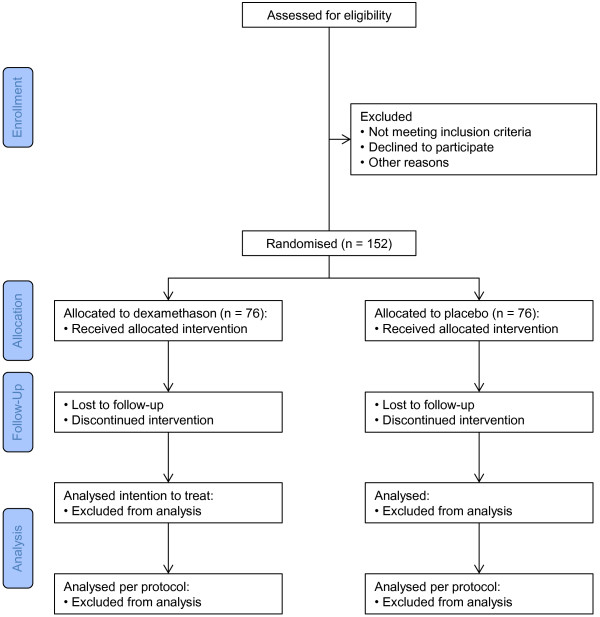
METHODS/DESIGN: We will perform a parallel two-arm, randomized (1:1), double-blind, placebo-controlled, single-center trial. Adults (≥18 years) scheduled for primary partial or total thyroidectomy because of a benign disease will be eligible for inclusion. The participants will be randomized to receive a single, intravenous preoperative dose of either 8 mg of dexamethasone in 2 ml saline (treatment group) or saline alone (placebo group). All the patients will receive a bilateral superficial cervical plexus block and standardized anesthesia. The primary outcome will be the incidence of postoperative nausea and vomiting. A total of 152 patients will be recruited, providing 80% power to detect a 50% reduction in the incidence of postoperative nausea and vomiting. Any patients who require opioid treatment will be excluded from the per-protocol analysis.
In the present protocol, we reduced bias to the greatest extent possible. Thus, we expect to definitively clarify the efficacy of dexamethasone for postoperative nausea and vomiting prophylaxis.
http://www.clinicaltrials.gov: NCT01189292.
全麻后恶心和呕吐不仅是一种影响 20-30%手术患者的令人不适的问题,还可能导致严重的术后并发症。甲状腺切除术后恶心和呕吐的发生率特别高。地塞米松在对抗化疗引起的恶心和呕吐方面被描述为非常有效,并被提议作为预防术后恶心和呕吐的一线方法。尽管有这种可能的有益效果,但在手术前预防性给予地塞米松以预防或减轻术后恶心和呕吐尚未得到证实。在全身麻醉下进行甲状腺手术时行双侧颈浅丛阻滞可显著减轻疼痛。更具临床意义的是,这种阻滞可避免术后需要使用阿片类药物。因此,接受甲状腺切除术和双侧颈浅丛阻滞的患者是研究地塞米松预防术后恶心和呕吐疗效的理想人群。这些患者术后恶心和呕吐发生率高,且无需使用阿片类药物。他们没有腹部手术,这可能通过麻痹性肠梗阻引起恶心和呕吐。结合我们机构使用的高度标准化的麻醉方案,这种设置可以控制所有已知的偏倚。
方法/设计:我们将进行一项平行、双臂、随机(1:1)、双盲、安慰剂对照、单中心试验。因良性疾病而接受原发性部分或全甲状腺切除术的成年人(≥18 岁)将有资格入组。参与者将被随机分为接受单次静脉注射 8mg 地塞米松加 2ml 生理盐水(治疗组)或单独生理盐水(安慰剂组)。所有患者将接受双侧颈浅丛阻滞和标准化麻醉。主要结局是术后恶心和呕吐的发生率。将招募 152 名患者,提供 80%的效力来检测术后恶心和呕吐发生率降低 50%。任何需要阿片类药物治疗的患者将被排除在方案外分析之外。
在本方案中,我们最大程度地减少了偏倚。因此,我们预计将明确地阐明地塞米松预防术后恶心和呕吐的疗效。