Ulrich Marcus, Department of Infectious Disease Epidemiology, Robert Koch-Institute, P,O, Box 650261, Berlin 13302, Germany.
BMC Public Health. 2013 Sep 10;13:826. doi: 10.1186/1471-2458-13-826.
Behavioural data from MSM are usually collected in non-representative convenience samples, increasingly on the internet. Epidemiological data from such samples might be useful for comparisons between countries, but are subject to unknown participation biases.
Self-reported HIV diagnoses from participants of the European MSM Internet Survey (EMIS) living in the Czech Republic, Germany, The Netherlands, Portugal, Sweden and the United Kingdom were compared with surveillance data, for both the overall diagnosed prevalence and for new diagnoses made in 2009. Country level prevalence and new diagnoses rates per 100 MSM were calculated based on an assumed MSM population size of 3% of the adult male population. Survey-surveillance discrepancies (SSD) for survey participation, diagnosed HIV prevalence and new HIV diagnoses were determined as ratios of proportions. Results are calculated and presented by 5-year age groups for MSM aged 15-64.
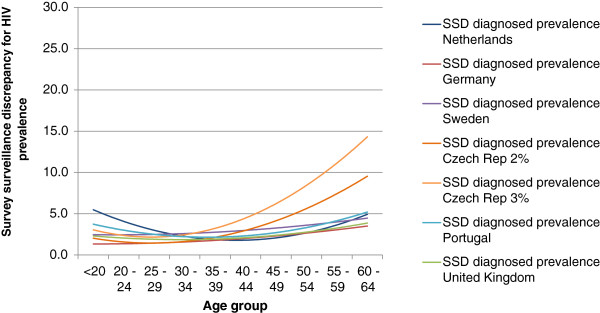
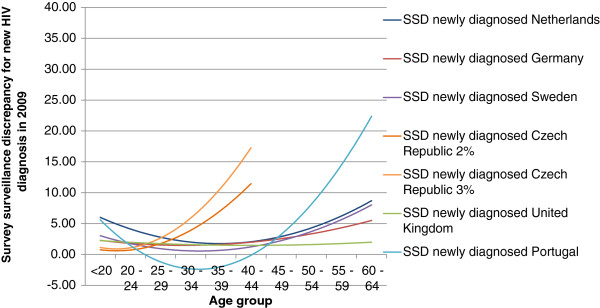
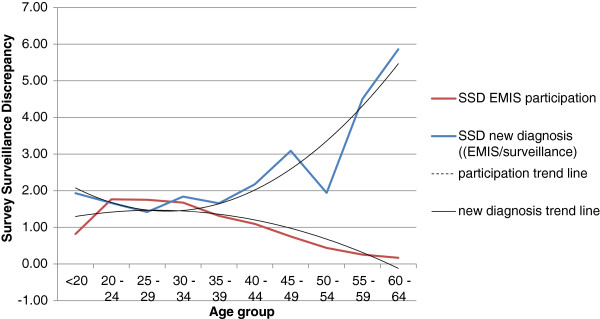
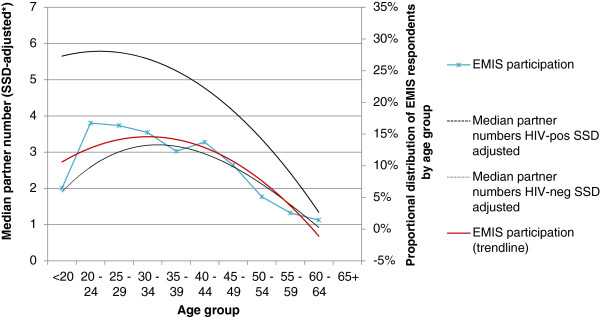
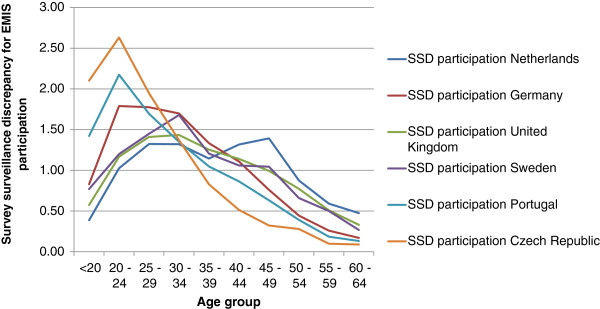
Surveillance derived estimates of diagnosed HIV prevalence among MSM aged 15-64 ranged from 0.63% in the Czech Republic to 4.93% in The Netherlands. New HIV diagnoses rates ranged between 0.10 per 100 MSM in the Czech Republic and 0.48 per 100 in The Netherlands. Self-reported rates from EMIS were consistently higher, with prevalence ranging from 2.68% in the Czech Republic to 12.72% in The Netherlands, and new HIV diagnoses rates from 0.36 per 100 in Sweden to 1.44 per 100 in The Netherlands. Across age groups, the survey surveillance discrepancies (SSD) for new HIV diagnoses were between 1.93 in UK and 5.95 in the Czech Republic, and for diagnosed prevalence between 1.80 in Germany and 4.26 in the Czech Republic.Internet samples of MSM were skewed towards younger age groups when compared to an age distribution of the general adult male population. Survey-surveillance discrepancies (SSD) for EMIS participation were inverse u-shaped across the age range. The two HIV-related SSD were u- or j-shaped with higher values for the very young and for older MSM. The highest discrepancies between survey and surveillance data regarding HIV-prevalence were observed in the oldest age group in Sweden and the youngest age group in Portugal.
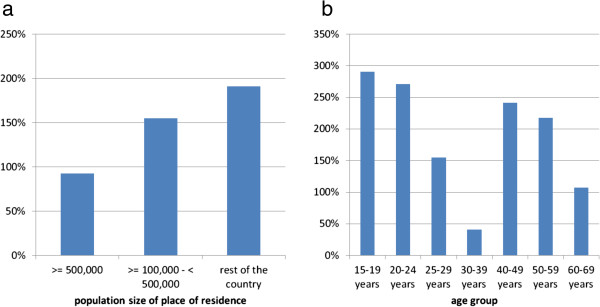
Internet samples are biased towards a lower median age because younger men are over-represented on MSM dating websites and therefore may be more likely to be recruited into surveys. Men diagnosed with HIV were over-represented in the internet survey, and increasingly so in the older age groups. A similar effect was observed in the age groups younger than 25 years. Self-reported peak prevalence and peak HIV diagnoses rates are often shifted to higher age groups in internet samples compared to surveillance data. Adjustment for age-effects on online accessibility should be considered when linking data from internet surveys with surveillance data.
男男性行为者(MSM)的行为数据通常来自于非代表性的便利样本,越来越多地来自互联网。来自此类样本的流行病学数据对于国家间的比较可能有用,但存在未知的参与偏差。
对居住在捷克共和国、德国、荷兰、葡萄牙、瑞典和英国的欧洲男男性行为者互联网调查(EMIS)参与者的自我报告的艾滋病毒诊断与监测数据进行了比较,同时比较了总体诊断流行率和 2009 年新诊断病例。根据成年男性人口中 3%的假设男男性行为者人口规模,计算了每个国家的流行率和每 100 名男男性行为者的新诊断病例率。通过比例确定了调查参与度、艾滋病毒诊断流行率和新艾滋病毒诊断的调查-监测差异(SSD)。结果以 15-64 岁男男性行为者的 5 岁年龄组为单位进行计算和呈现。
15-64 岁男男性行为者中,监测数据显示艾滋病毒诊断流行率从捷克共和国的 0.63%到荷兰的 4.93%不等。新艾滋病毒诊断率在捷克共和国为 0.10 例/100 名男男性行为者,在荷兰为 0.48 例/100 名男男性行为者。EMIS 自我报告的比例始终较高,从捷克共和国的 2.68%到荷兰的 12.72%,新艾滋病毒诊断率从瑞典的 0.36 例/100 名男男性行为者到荷兰的 1.44 例/100 名男男性行为者。在不同年龄组中,新艾滋病毒诊断的调查-监测差异(SSD)在英国为 1.93,在捷克共和国为 5.95,艾滋病毒诊断流行率的 SSD 在德国为 1.80,在捷克共和国为 4.26。与普通成年男性人口的年龄分布相比,MSM 的互联网样本偏向于年轻年龄组。EMIS 参与度的调查-监测差异(SSD)在整个年龄范围内呈反 U 形。两个与艾滋病毒相关的 SSD 呈 U 形或 J 形,年轻和年长 MSM 的值较高。在瑞典,年龄最大的年龄组和葡萄牙年龄最小的年龄组中,艾滋病毒流行率的调查数据与监测数据之间的差异最大。
互联网样本偏向于较低的中位数年龄,因为年轻男性在男男性接触者约会网站上的代表性过高,因此更有可能被招募参与调查。艾滋病毒诊断男性在互联网调查中比例过高,而且在年龄较大的年龄组中比例越来越高。在 25 岁以下的年龄组中也观察到了类似的影响。与监测数据相比,互联网样本中自我报告的峰值流行率和峰值艾滋病毒诊断率往往转移到更高的年龄组。在将互联网调查数据与监测数据联系起来时,应考虑年龄对在线可及性的影响进行调整。