Department of Pathology and Laboratory Medicine, University of British Columbia, Vancouver, British Columbia, Canada.
PLoS One. 2013 Sep 4;8(9):e72162. doi: 10.1371/journal.pone.0072162. eCollection 2013.
OVARIAN CARCINOMAS CONSIST OF AT LEAST FIVE DISTINCT DISEASES: high-grade serous, low-grade serous, clear cell, endometrioid, and mucinous. Biomarker and molecular characterization may represent a more biologically relevant basis for grouping and treating this family of tumors, rather than site of origin. Molecular characteristics have become the new standard for clinical pathology, however development of tailored type-specific therapies is hampered by a failure of basic research to recognize that model systems used to study these diseases must also be stratified. Unrelated model systems do offer value for study of biochemical processes but specific cellular context needs to be applied to assess relevant therapeutic strategies.
We have focused on the identification of clear cell carcinoma cell line models. A panel of 32 "ovarian cancer" cell lines has been classified into histotypes using a combination of mutation profiles, IHC mutation-surrogates, and a validated immunohistochemical model. All cell lines were identity verified using STR analysis.
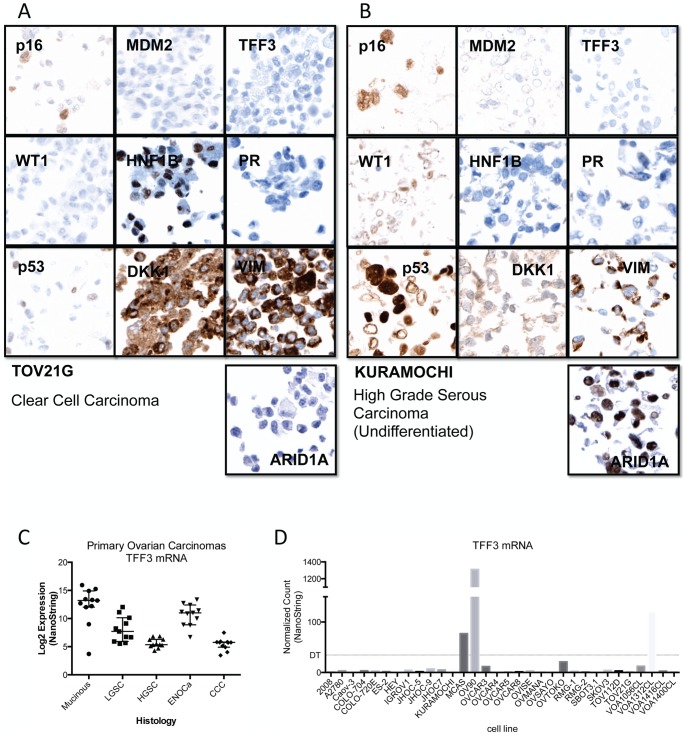
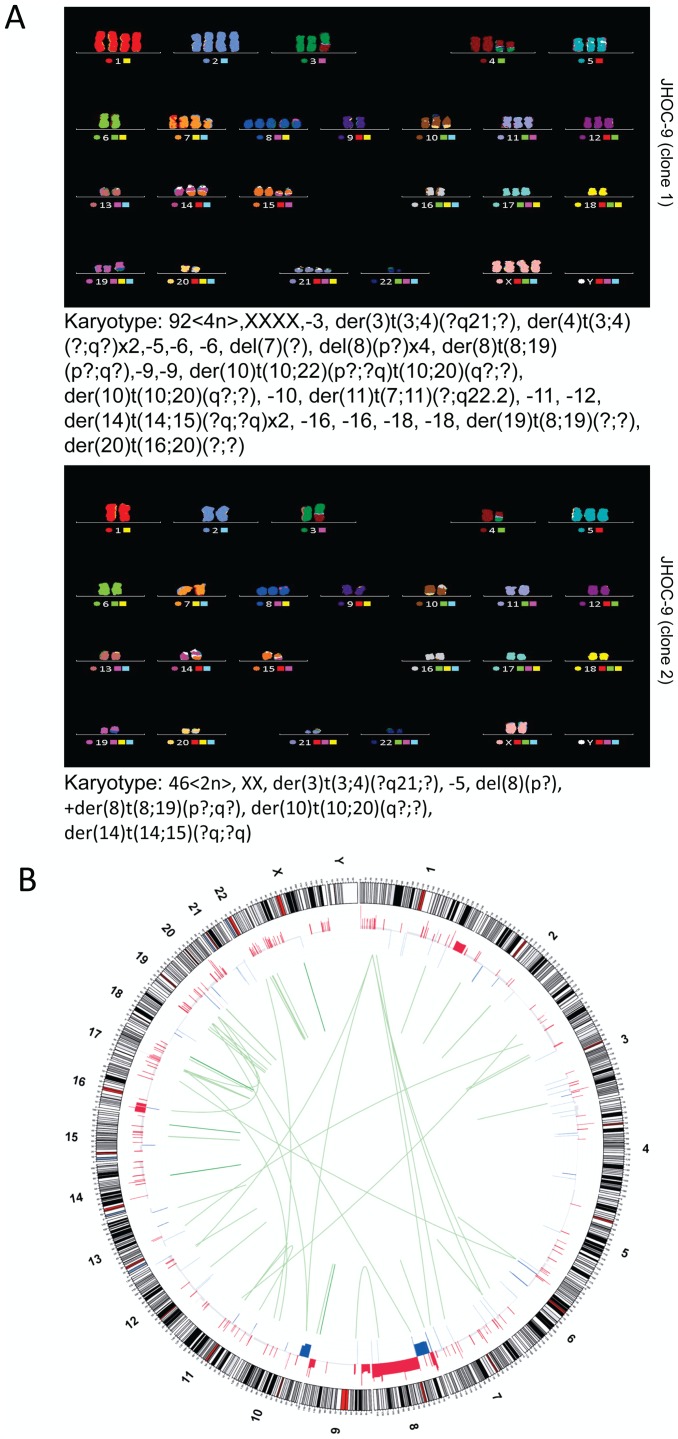
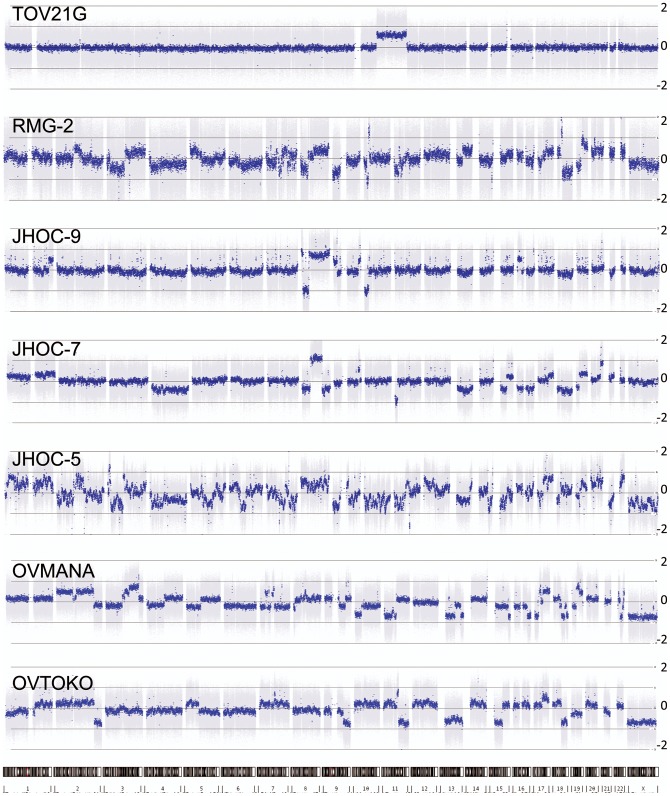
Many described ovarian clear cell lines have characteristic mutations (including ARID1A and PIK3CA) and an overall molecular/immuno-profile typical of primary tumors. Mutations in TP53 were present in the majority of high-grade serous cell lines. Advanced genomic analysis of bona-fide clear cell carcinoma cell lines also support copy number changes in typical biomarkers such at MET and HNF1B and a lack of any recurrent expressed re-arrangements.
As with primary ovarian tumors, mutation status of cancer genes like ARID1A and TP53 and a general immuno-profile serve well for establishing histotype of ovarian cancer cell We describe specific biomarkers and molecular features to re-classify generic "ovarian carcinoma" cell lines into type specific categories. Our data supports the use of prototype clear cell lines, such as TOV21G and JHOC-5, and questions the use of SKOV3 and A2780 as models of high-grade serous carcinoma.
卵巢癌至少包括五种不同的疾病:高级别浆液性癌、低级别浆液性癌、透明细胞癌、子宫内膜样癌和黏液性癌。生物标志物和分子特征可能代表了对这种肿瘤家族进行分组和治疗的更具生物学意义的基础,而不是起源部位。分子特征已成为临床病理学的新标准,然而,基础研究未能认识到用于研究这些疾病的模型系统也需要分层,这阻碍了针对特定类型的治疗方法的开发。不相关的模型系统确实为生化过程的研究提供了价值,但需要应用特定的细胞环境来评估相关的治疗策略。
我们专注于鉴定透明细胞癌细胞系模型。使用突变谱、免疫组化突变替代物和经过验证的免疫组织化学模型的组合,对 32 种“卵巢癌”细胞系进行了组织型分类。所有细胞系均使用 STR 分析进行身份验证。
许多描述的卵巢透明细胞系具有特征性突变(包括 ARID1A 和 PIK3CA),并且具有与原发性肿瘤相似的整体分子/免疫表型。大多数高级别浆液性细胞系中存在 TP53 突变。对真正的透明细胞癌细胞系的高级基因组分析也支持典型生物标志物如 MET 和 HNF1B 的拷贝数变化,以及缺乏任何反复出现的表达重排。
与原发性卵巢肿瘤一样,癌症基因如 ARID1A 和 TP53 的突变状态以及一般的免疫表型对于确定卵巢癌细胞的组织型非常有效。我们描述了特定的生物标志物和分子特征,可将通用的“卵巢癌”细胞系重新分类为特定类型的类别。我们的数据支持使用原型透明细胞系,如 TOV21G 和 JHOC-5,并对使用 SKOV3 和 A2780 作为高级别浆液性癌模型提出了质疑。