University of Gothenburg.
J Appl Clin Med Phys. 2013 Sep 6;14(5):127-39. doi: 10.1120/jacmp.v14i5.4316.
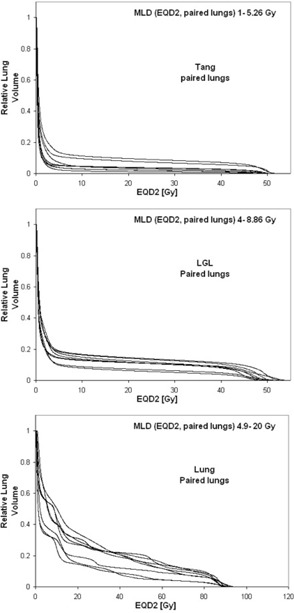
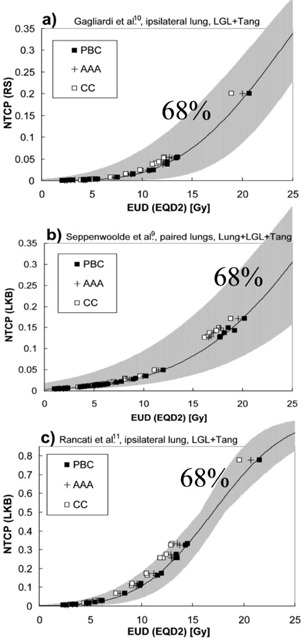
Due to limitations and uncertainties in dose calculation algorithms, different algorithms can predict different dose distributions and dose-volume histograms for the same treatment. This can be a problem when estimating the normal tissue complication probability (NTCP) for patient-specific dose distributions. Published NTCP model parameters are often derived for a different dose calculation algorithm than the one used to calculate the actual dose distribution. The use of algorithm-specific NTCP model parameters can prevent errors caused by differences in dose calculation algorithms. The objective of this work was to determine how to change the NTCP model parameters for lung complications derived for a simple correction-based pencil beam dose calculation algorithm, in order to make them valid for three other common dose calculation algorithms. NTCP was calculated with the relative seriality (RS) and Lyman-Kutcher-Burman (LKB) models. The four dose calculation algorithms used were the pencil beam (PB) and collapsed cone (CC) algorithms employed by Oncentra, and the pencil beam convolution (PBC) and anisotropic analytical algorithm (AAA) employed by Eclipse. Original model parameters for lung complications were taken from four published studies on different grades of pneumonitis, and new algorithm-specific NTCP model parameters were determined. The difference between original and new model parameters was presented in relation to the reported model parameter uncertainties. Three different types of treatments were considered in the study: tangential and locoregional breast cancer treatment and lung cancer treatment. Changing the algorithm without the derivation of new model parameters caused changes in the NTCP value of up to 10 percentage points for the cases studied. Furthermore, the error introduced could be of the same magnitude as the confidence intervals of the calculated NTCP values. The new NTCP model parameters were tabulated as the algorithm was varied from PB to PBC, AAA, or CC. Moving from the PB to the PBC algorithm did not require new model parameters; however, moving from PB to AAA or CC did require a change in the NTCP model parameters, with CC requiring the largest change. It was shown that the new model parameters for a given algorithm are different for the different treatment types.
由于剂量计算算法的局限性和不确定性,对于相同的治疗方案,不同的算法可能会预测出不同的剂量分布和剂量-体积直方图。当估计特定于患者的剂量分布的正常组织并发症概率 (NTCP) 时,这可能会成为一个问题。已发表的 NTCP 模型参数通常是针对与实际剂量分布计算中使用的算法不同的算法推导得出的。使用特定于算法的 NTCP 模型参数可以防止因剂量计算算法的差异而导致的错误。本研究的目的是确定如何更改为简单的基于校正的笔束剂量计算算法推导得出的用于肺部并发症的 NTCP 模型参数,以便使其适用于另外三种常见的剂量计算算法。使用相对序列性 (RS) 和 Lyman-Kutcher-Burman (LKB) 模型计算 NTCP。使用的四种剂量计算算法是 Oncentra 采用的笔束 (PB) 和崩溃圆锥 (CC) 算法,以及 Eclipse 采用的笔束卷积 (PBC) 和各向异性解析算法 (AAA)。原始的肺部并发症模型参数取自四项关于不同等级的放射性肺炎的已发表研究,确定了新的特定于算法的 NTCP 模型参数。以报告的模型参数不确定性为参考,呈现了原始模型参数与新模型参数之间的差异。研究中考虑了三种不同类型的治疗:切线和局部区域乳腺癌治疗和肺癌治疗。在不推导新模型参数的情况下改变算法会导致所研究病例的 NTCP 值发生高达 10 个百分点的变化。此外,引入的误差可能与计算的 NTCP 值的置信区间大小相当。随着算法从 PB 变为 PBC、AAA 或 CC,新的 NTCP 模型参数被制成表格。从 PB 到 PBC 算法的移动不需要新的模型参数;然而,从 PB 到 AAA 或 CC 的移动确实需要更改 NTCP 模型参数,其中 CC 需要最大的更改。结果表明,对于不同的治疗类型,给定算法的新模型参数是不同的。