aAlbert Einstein College of Medicine/Montefiore Medical Center, Bronx, New York bRutgers University, Piscataway, New Jersey cSchool of Health Sciences and Practice/New York Medical College, Valhalla, New York dCook County Health and Hospitals System eRush University, Chicago, Illinois fUniversity of California San Francisco, San Francisco, California gJohns Hopkins Bloomberg School of Public Health, Baltimore, Maryland hState University of New York/Downstate Medical Center, Brooklyn, New York, USA iUniversity of Gothenburg, Gothenburg, Sweden jUniversity of Southern California, Los Angeles, California kGeorgetown University, Washington, District of Columbia, USA.
AIDS. 2013 Sep 24;27(15):2413-23. doi: 10.1097/01.aids.0000432537.92958.73.
To assess the association of race with clinical outcomes in HIV-positive women on continuous HAART.
Prospective study that enrolled women from 1994 to 1995 and 2001 to 2002.
Women's Interagency HIV Study, a community-based cohort in five US cities.
One thousand, four hundred and seventy-one HIV-positive continuous HAART users.
Times to AIDS and non-AIDS death and incident AIDS-defining illness (ADI) after HAART initiation.
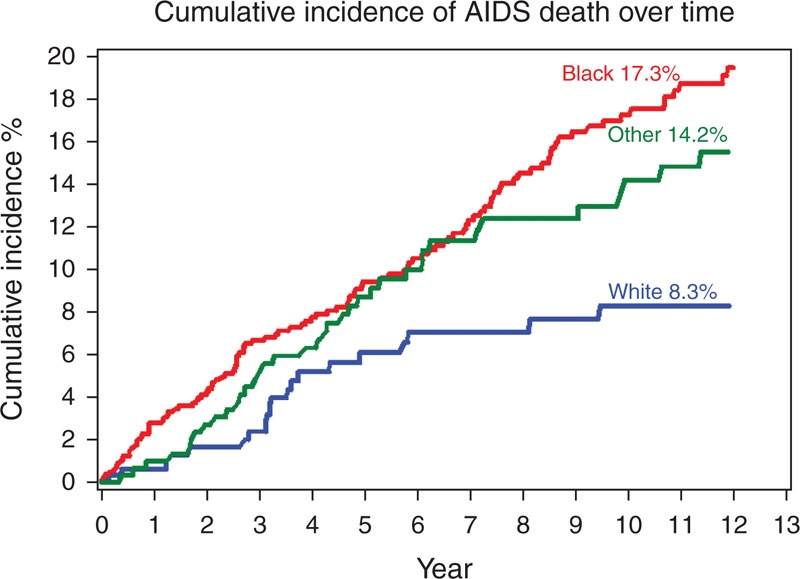
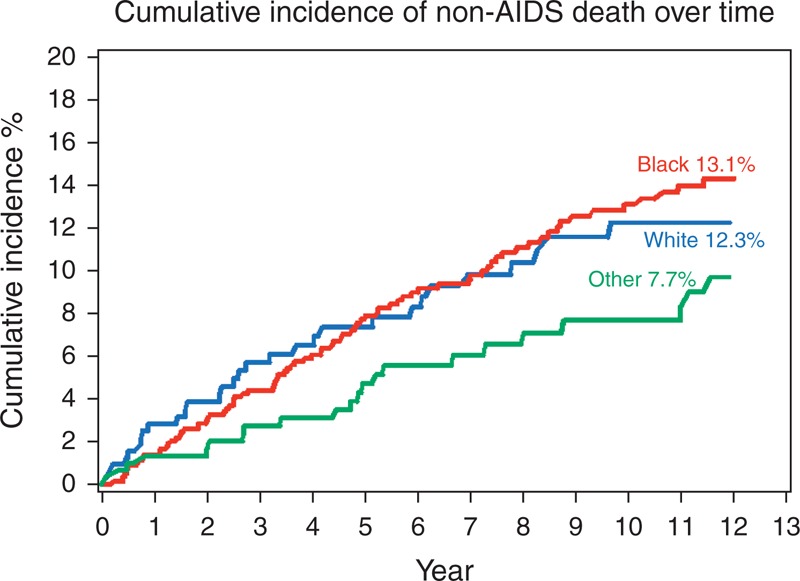
In adjusted analyses, black vs. white women had higher rates of AIDS death [adjusted hazard ratio (aHR) 2.14, 95% confidence interval (CI) 1.30, 3.50; P = 0.003] and incident ADI (aHR 1.58, 95% CI 1.08, 2.32; P = 0.02), but not non-AIDS death (aHR 0.91, 95% CI 0.59, 1.39; P = 0.65). Cumulative AIDS death incidence at 10 years was 17.3 and 8.3% for black and white women, respectively. Other significant independent pre-HAART predictors of AIDS death included peak viral load (aHR 1.70 per log₁₀, 95% CI 1.34, 2.16; P < 0.001), nadir CD4⁺ cell count (aHR 0.65 per 100 cells/μl, 95% CI 0.56, 0.76; P < 0.001), depressive symptoms by Center for Epidemiology Studies Depression score at least 16 (aHR 2.10, 95% CI 1.51, 2.92; P < 0.001), hepatitis C virus infection (aHR 1.57, 95% CI 1.02, 2.40; P = 0.04), and HIV acquisition via transfusion (aHR 2.33, 95% CI 1.21, 4.49; P = 0.01). In models with time-updated HAART adherence, association of race with AIDS death remained statistically significant (aHR 3.09, 95% CI 1.38, 6.93; P = 0.006).
In continuous HAART-using women, black women more rapidly died from AIDS or experienced incident ADI than their white counterparts after adjusting for confounders. Future studies examining behavioral and biologic factors in these women may further the understanding of HAART prognosis.
评估在持续使用高效抗逆转录病毒治疗(HAART)的 HIV 阳性女性中,种族与临床结局的相关性。
前瞻性研究,纳入了 1994 年至 1995 年和 2001 年至 2002 年的女性。
妇女艾滋病联合研究,美国五个城市的一个基于社区的队列。
1471 名持续使用 HAART 的 HIV 阳性连续使用者。
HAART 开始后艾滋病和非艾滋病死亡以及艾滋病定义性疾病(ADI)的发生时间。
在调整后的分析中,与白人女性相比,黑人女性的艾滋病死亡[调整后的危险比(aHR)2.14,95%置信区间(CI)1.30,3.50;P=0.003]和发生 ADI(aHR 1.58,95%CI 1.08,2.32;P=0.02)的发生率更高,但非艾滋病死亡(aHR 0.91,95%CI 0.59,1.39;P=0.65)的发生率没有差异。10 年内黑人女性的累积 AIDS 死亡率为 17.3%,白人女性为 8.3%。艾滋病死亡的其他重要独立的 HAART 前预测因素包括峰值病毒载量(aHR 每 log₁₀增加 1.70,95%CI 1.34,2.16;P<0.001)、最低点 CD4+细胞计数(aHR 每 100 个细胞/μl 减少 0.65,95%CI 0.56,0.76;P<0.001)、中心流行病学研究抑郁评分至少为 16 的抑郁症状(aHR 2.10,95%CI 1.51,2.92;P<0.001)、丙型肝炎病毒感染(aHR 1.57,95%CI 1.02,2.40;P=0.04)和通过输血获得 HIV(aHR 2.33,95%CI 1.21,4.49;P=0.01)。在包含时间更新的 HAART 依从性的模型中,种族与艾滋病死亡的相关性在统计学上仍然显著(aHR 3.09,95%CI 1.38,6.93;P=0.006)。
在持续使用 HAART 的女性中,黑人女性比白人女性更快地死于艾滋病或出现 ADI,这在调整了混杂因素后仍然具有统计学意义。未来研究在这些女性中进一步探讨行为和生物学因素,可能有助于进一步了解 HAART 的预后。