Department of Internal Medicine, School of Medicine, Universidad de Antioquia, Medellín AA 1226, Colombia.
BMC Anesthesiol. 2013 Sep 19;13(1):23. doi: 10.1186/1471-2253-13-23.
Given the acknowledged problems in sepsis diagnosis, we use a novel way with the application of the latent class analysis (LCA) to determine the operative characteristics of C-reactive protein (CRP), D-dimer (DD) and Procalcitonin (PCT) as diagnostic tests for sepsis in patients admitted to hospital care with a presumptive infection.
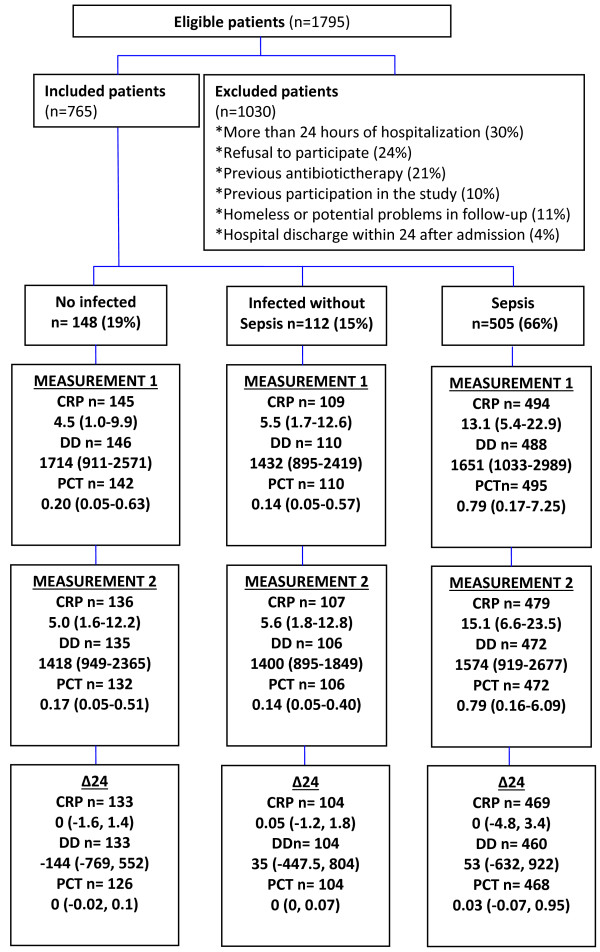
Cross-sectional study to determine the diagnostic accuracy of three biological markers against the gold standard of clinical definition of sepsis provided by an expert committee, and also against the likelihood of sepsis according to LCA. Patients were recruited in the emergency room within 24 hours of hospitalization and were follow-up daily until discharge.
Among 765 patients, the expert committee classified 505 patients (66%) with sepsis, 112 (15%) with infection but without sepsis and 148 (19%) without infection. The best cut-offs points for CRP, DD, and PCT were 7.8 mg/dl, 1616 ng/ml and 0.3 ng/ml, respectively; but, neither sensitivity nor specificity reach 70% for any biomarker. The LCA analysis with the same three tests identified a "cluster" of 187 patients with several characteristics suggesting a more severe condition as well as better microbiological confirmation. Assuming this subset of patients as the new prevalence of sepsis, the ROC curve analysis identified new cut-off points for the tests and suggesting a better discriminatory ability for PCT with a value of 2 ng/ml.
Under a "classical" definition of sepsis three typical biomarkers (CRP, PCT and DD) are not capable enough to differentiate septic from non-septic patients in the ER. However, a higher level of PCT discriminates a selected group of patients with severe sepsis.
鉴于脓毒症诊断中存在公认的问题,我们采用一种新的方法,应用潜在类别分析(LCA)来确定 C 反应蛋白(CRP)、D-二聚体(DD)和降钙素原(PCT)作为疑似感染住院患者脓毒症的诊断试验的操作特征。
本横断面研究旨在确定三种生物标志物对脓毒症临床定义的金标准(由专家委员会提供)的诊断准确性,以及对 LCA 预测脓毒症可能性的诊断准确性。患者在入院后 24 小时内于急诊室入组,并在住院期间每天进行随访直至出院。
在 765 例患者中,专家委员会将 505 例(66%)患者分类为脓毒症,112 例(15%)患者为感染但无脓毒症,148 例(19%)患者为无感染。CRP、DD 和 PCT 的最佳截断值分别为 7.8mg/dl、1616ng/ml 和 0.3ng/ml;但任何一种生物标志物的敏感性和特异性均未达到 70%。采用相同的三种检测方法进行 LCA 分析,确定了一个具有多个特征的“簇”,这些特征提示患者病情更严重,微生物学证据更好。假设该亚组患者的脓毒症患病率发生变化,那么 ROC 曲线分析确定了这些检测方法的新截断值,并表明 PCT 的鉴别能力更好,截断值为 2ng/ml。
在脓毒症的“经典”定义下,三种典型的生物标志物(CRP、PCT 和 DD)无法区分急诊室中的脓毒症患者和非脓毒症患者。然而,较高水平的 PCT 可以区分一组严重脓毒症患者。