Ma Huiyan, Lu Yani, Marchbanks Polly A, Folger Suzanne G, Strom Brian L, McDonald Jill A, Simon Michael S, Weiss Linda K, Malone Kathleen E, Burkman Ronald T, Sullivan-Halley Jane, Deapen Dennis M, Press Michael F, Bernstein Leslie
Breast Cancer Res. 2013;15(5):R90. doi: 10.1186/bcr3486.
The association of breast cancer patients’ mortality with estrogen receptor (ER) status (ER + versus ER-) has been well studied. However, little attention has been paid to the relationship between the quantitative measures of ER expression and mortality.
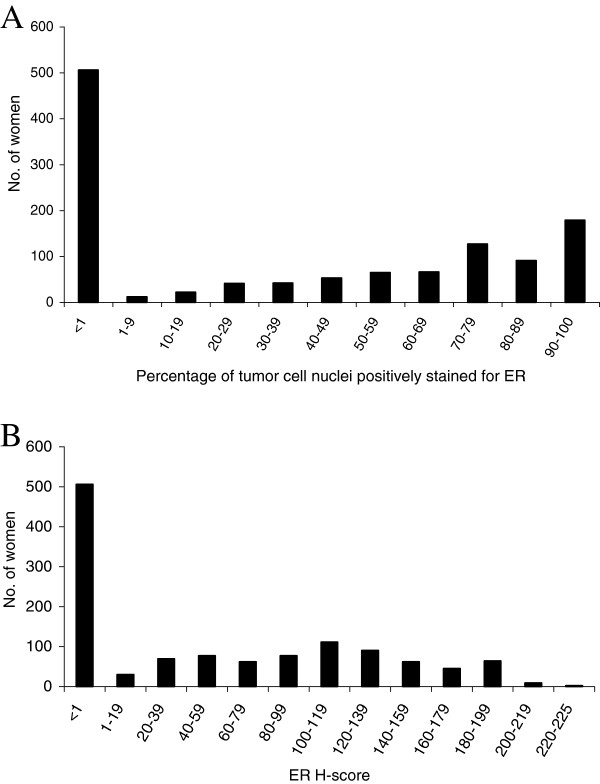
We evaluated the association between semi-quantitative, immunohistochemical staining of ER in formalin-fixed paraffin-embedded breast carcinomas and breast cancer-specific mortality risk in an observational cohort of invasive breast cancer in 681 white women and 523 black women ages 35-64 years at first diagnosis of invasive breast cancer, who were followed for a median of 10 years. The quantitative measures of ER examined here included the percentage of tumor cell nuclei positively stained for ER, ER Histo (H)-score, and a score based on an adaptation of an equation presented by Cuzick and colleagues, which combines weighted values of ER H-score, percentage of tumor cell nuclei positively stained for the progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) results. This is referred to as the ER/PR/HER2 score.
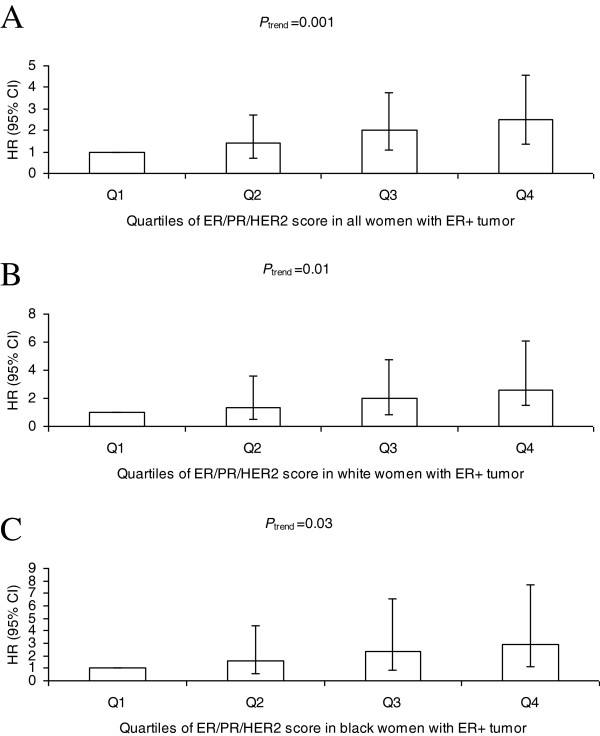
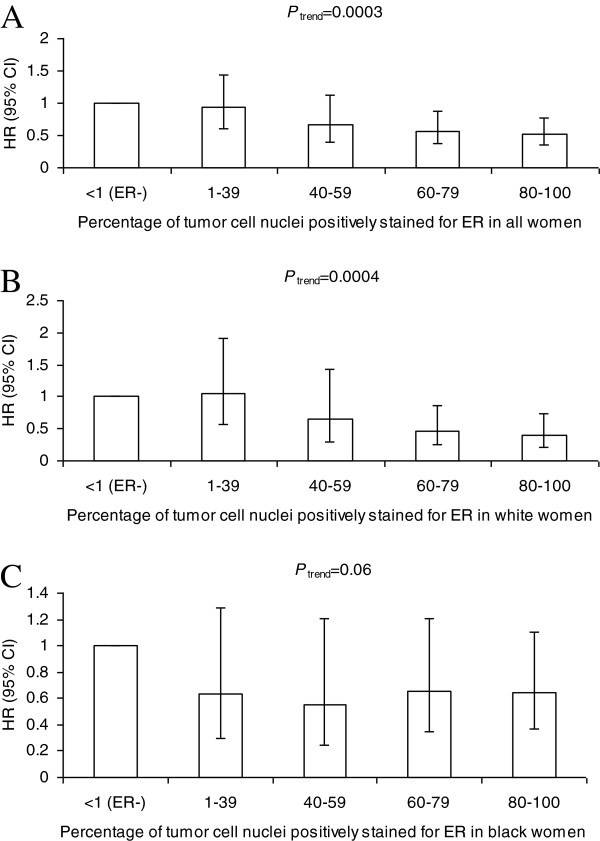
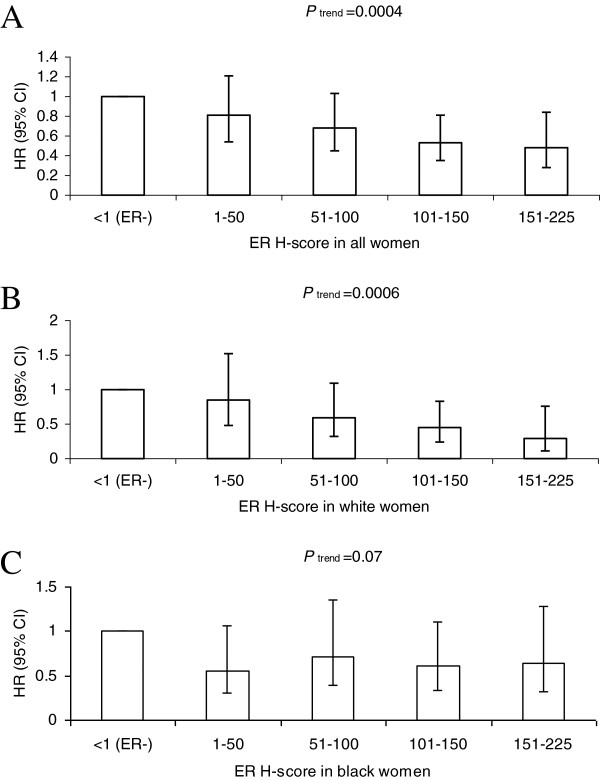
After controlling for age at diagnosis, race, study site, tumor stage, and histologic grade in multivariable Cox proportional hazards regression models, both percentage of tumor cell nuclei positively stained for ER (Ptrend = 0.0003) and the ER H-score (Ptrend = 0.0004) were inversely associated with breast cancer-specific mortality risk. The ER/PR/HER2 score was positively associated with breast cancer-specific mortality risk in women with ER + tumor (Ptrend = 0.001). Analyses by race revealed that ER positivity was associated with reduced risk of breast cancer-specific mortality in white women and black women. The two quantitative measures for ER alone provided additional discrimination in breast cancer-specific mortality risk only among white women with ER + tumors (both Ptrend ≤ 0.01) while the ER/PR/HER2 score provided additional discrimination for both white women (Ptrend = 0.01) and black women (Ptrend = 0.03) with ER + tumors.
Our data support quantitative immunohistochemical measures of ER, especially the ER/PR/HER2 score, as a more precise predictor for breast cancer-specific mortality risk than a simple determination of ER positivity.
乳腺癌患者死亡率与雌激素受体(ER)状态(ER阳性与ER阴性)之间的关联已得到充分研究。然而,ER表达的定量测量与死亡率之间的关系却很少受到关注。
我们评估了在681名白人女性和523名黑人女性组成的浸润性乳腺癌观察队列中,福尔马林固定石蜡包埋乳腺癌组织中ER的半定量免疫组化染色与乳腺癌特异性死亡风险之间的关联。这些女性在首次诊断为浸润性乳腺癌时年龄在35至64岁之间,中位随访时间为10年。此处检测的ER定量测量指标包括ER阳性染色的肿瘤细胞核百分比、ER组织学(H)评分,以及基于Cuzick及其同事提出的一个公式改编的评分,该公式结合了ER H评分的加权值、孕激素受体(PR)阳性染色的肿瘤细胞核百分比和人表皮生长因子受体2(HER2)结果。这被称为ER/PR/HER2评分。
在多变量Cox比例风险回归模型中,控制了诊断年龄、种族、研究地点、肿瘤分期和组织学分级后,ER阳性染色的肿瘤细胞核百分比(Ptrend = 0.0003)和ER H评分(Ptrend = 0.0004)均与乳腺癌特异性死亡风险呈负相关。在ER阳性肿瘤的女性中,ER/PR/HER2评分与乳腺癌特异性死亡风险呈正相关(Ptrend = 0.001)。按种族分析显示,ER阳性与白人女性和黑人女性乳腺癌特异性死亡风险降低相关。仅ER的两种定量测量指标仅在ER阳性肿瘤的白人女性中对乳腺癌特异性死亡风险提供了额外的区分能力(两者Ptrend≤0.01),而ER/PR/HER2评分对ER阳性肿瘤的白人女性(Ptrend = 0.01)和黑人女性(Ptrend = 0.03)均提供了额外的区分能力。
我们的数据支持ER的定量免疫组化测量,尤其是ER/PR/HER2评分,作为比简单确定ER阳性更精确的乳腺癌特异性死亡风险预测指标。