Majumdar Sumit R, Hemmelgarn Brenda R, Lin Meng, McBrien Kerry, Manns Braden J, Tonelli Marcello
Corresponding author: Marcello Tonelli,
Diabetes Care. 2013 Nov;36(11):3585-90. doi: 10.2337/dc13-0523. Epub 2013 Oct 2.
Little is known about the prognostic impact of hypoglycemia associated with hospitalization. We hypothesized that hospitalized hypoglycemia would be associated with increased long-term morbidity and mortality, irrespective of diabetes status.
We undertook a cohort study using linked administrative health care and laboratory databases in Alberta, Canada. From 1 January 2004 to 31 March 2009, we included all outpatients 66 years of age and older who had at least one serum creatinine and one A1C measured. To examine the independent association between hospitalized hypoglycemia and all-cause mortality, we used time-varying Cox proportional hazards (adjusted hazard ratio [aHR]), and for all-cause hospitalizations, we used Poisson regression (adjusted incidence rate ratio [aIRR]).
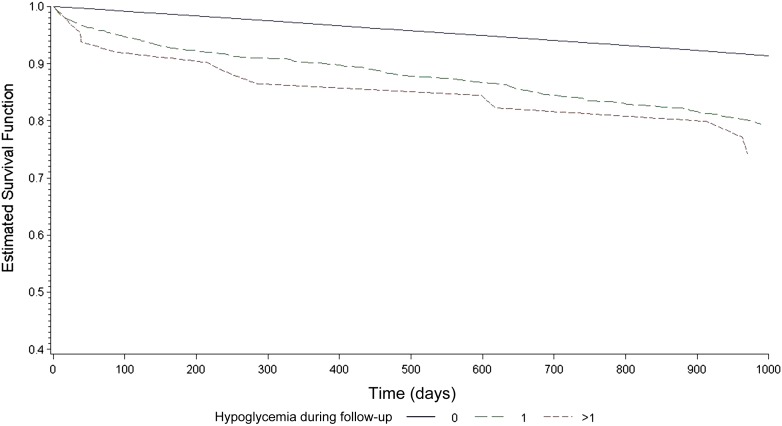
The cohort included 85,810 patients: mean age 75 years, 51% female, and 50% had diabetes defined by administrative data. Overall, 440 patients (0.5%) had severe hypoglycemia associated with hospitalization and most (93%) had diabetes. During 4 years of follow-up, 16,320 (19%) patients died. Hospitalized hypoglycemia was independently associated with increased mortality (60 vs. 19% mortality for no hypoglycemia; aHR 2.55 [95% CI 2.25-2.88]), and this increased in a dose-dependent manner (aHR no hypoglycemia = 1.0 vs. one episode = 2.49 vs. one or more = 3.78, P trend <0.001). Hospitalized hypoglycemia was also independently associated with subsequent hospitalizations (aIRR no hypoglycemia = 1.0 vs. one episode = 1.90 vs. one or more = 2.61, P trend <0.001) and recurrent hypoglycemia (aHR no hypoglycemia = 1.0 vs. one episode = 2.45 vs. one or more = 9.66, P trend <0.001).
Older people who have an episode of hospitalized hypoglycemia are easily identified and at substantially increased risk of morbidity and mortality.
关于与住院相关的低血糖的预后影响,人们了解甚少。我们推测,住院期间发生的低血糖与长期发病率和死亡率增加相关,无论糖尿病状态如何。
我们利用加拿大艾伯塔省的行政医疗保健和实验室数据库进行了一项队列研究。从2004年1月1日至2009年3月31日,我们纳入了所有66岁及以上且至少测量过一次血清肌酐和糖化血红蛋白(A1C)的门诊患者。为了研究住院低血糖与全因死亡率之间的独立关联,我们使用了时变Cox比例风险模型(调整后风险比[aHR]);对于全因住院情况,我们使用了泊松回归(调整后发病率比[aIRR])。
该队列包括85,810名患者:平均年龄75岁,51%为女性,行政数据定义的糖尿病患者占50%。总体而言,440名患者(0.5%)发生了与住院相关的严重低血糖,其中大多数(93%)患有糖尿病。在4年的随访期间,16,320名(19%)患者死亡。住院低血糖与死亡率增加独立相关(无低血糖者死亡率为19%,低血糖者为60%;aHR 2.55[95%置信区间2.25 - 2.88]),且呈剂量依赖性增加(无低血糖者aHR = 1.0,一次发作aHR = 2.49,一次或多次发作aHR = 3.78,P趋势<0.001)。住院低血糖还与随后的住院治疗独立相关(无低血糖者aIRR = 1.0,一次发作aIRR = 1.90,一次或多次发作aIRR = 2.61,P趋势<0.001)以及复发性低血糖(无低血糖者aHR = 1.0,一次发作aHR = 2.45,一次或多次发作aHR = 9.66,P趋势<0.001)。
发生过住院低血糖的老年人很容易被识别出来,其发病和死亡风险大幅增加。