Janssen Research and Development, LLC, Raritan, NJ, USA.
Neuropsychiatr Dis Treat. 2013;9:1381-92. doi: 10.2147/NDT.S49944. Epub 2013 Sep 20.
The purpose of this study was to compare incidence rates and time course of extrapyramidal symptom (EPS)-related treatment-emergent adverse events (TEAEs) between oral and long-acting injectable (LAI) paliperidone.
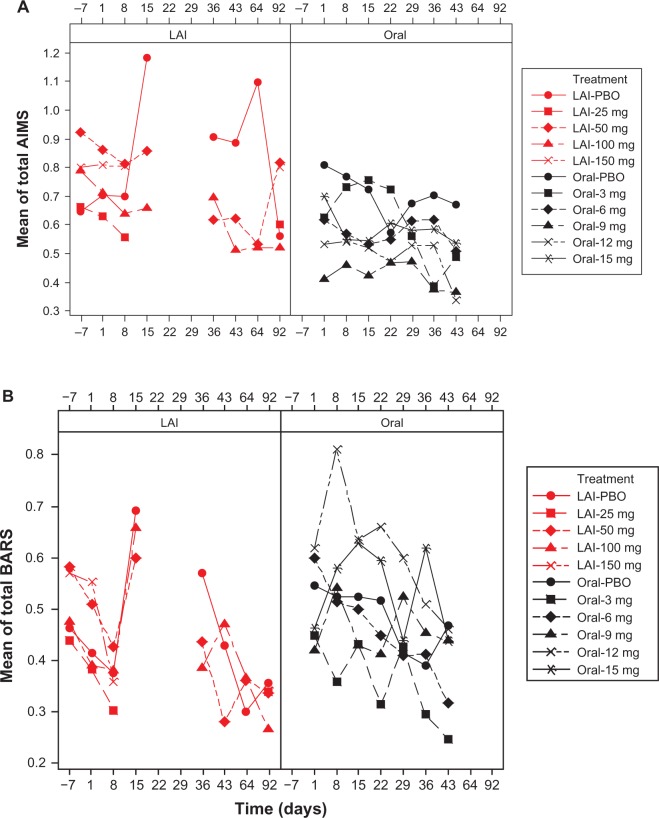
The analysis included pooled data (safety analysis set, 2,256 antipsychotic-treated and 865 placebo-treated patients with schizophrenia) from seven randomized, double-blind, placebo-controlled paliperidone studies (three oral [6 weeks each] and four LAI [9-13 weeks]) and assessed comparable doses (oral, 3-15 mg; LAI, 25-150 mg eq. [US doses 39-234 mg]). We summarized incidence rates and time of onset for EPS-related TEAE, categorized by EPS group terms, ie, tremor, dystonia, hyperkinesia, parkinsonism, and dyskinesia, and use of anti-EPS medication. Mean scores over time for the Abnormal Involuntary Movement Scale (AIMS, for dyskinesia), Barnes Akathisia Rating Scale (BARS, for akathisia), and Simpson Angus Rating Scale (SAS, for parkinsonism) were graphed.
Incidence rates for all categories of spontaneously reported EPS-related TEAEs except for hyperkinesia, were numerically lower in pooled LAI studies than in pooled oral studies. Highest rates were observed in the first week of paliperidone-LAI (for all EPS symptoms except dyskinesia) and oral paliperidone treatment (except parkinsonism and tremor). Anti-EPS medication use was significantly lower in LAI (12%) versus oral studies (17%, P = 0.0035). Mean values for EPS scale scores were similar between LAI and oral treatment at endpoint, and no dose response was evident. Mean reductions (standard deviation) from baseline to endpoint in EPS scale scores were larger for LAI (AIMS, -0.10 [1.27]; BARS, -0.09 [1.06]; SAS, -0.04 [0.20]) versus oral studies (AIMS, -0.08 [1.32]; BARS, -0.03 [1.24]; SAS, 0.0 [0.23]). These changes favored LAI for BARS (P = 0.023) and SAS (P < 0.0001), but not for AIMS (P = 0.49), at endpoint for the studies.
In this posthoc descriptive analysis, incidence rates of spontaneously reported EPS-related TEAEs were numerically lower following approximately 90 days of exposure with LAI and approximately 40 days with oral paliperidone at comparable doses.
本研究旨在比较口服和长效注射(LAI)帕利哌酮治疗精神分裂症患者时,与锥体外系症状(EPS)相关的治疗中出现的不良事件(TEAE)的发生率和时间进程。
该分析纳入了来自 7 项随机、双盲、安慰剂对照的帕利哌酮研究(3 项口服[各 6 周]和 4 项 LAI[9-13 周])的汇总数据(安全性分析集,2256 名接受抗精神病药物治疗和 865 名接受安慰剂治疗的精神分裂症患者),并评估了可比剂量(口服:3-15mg;LAI:25-150mg eq.[美国剂量 39-234mg])。我们按 EPS 组术语(震颤、肌张力障碍、运动障碍、帕金森病和运动障碍)总结了与 EPS 相关的 TEAEs 的发生率和发病时间,并对其进行了分类,同时还对使用抗 EPS 药物的情况进行了总结。使用异常不自主运动量表(AIMS,用于评估运动障碍)、巴恩斯静坐不安评定量表(BARS,用于评估静坐不能)和辛普森-安格斯帕金森病评定量表(SAS,用于评估帕金森病)的评分随时间变化的均值进行了绘制。
除运动障碍外,所有自发报告的与 EPS 相关的 TEAEs 类别中,汇总的 LAI 研究中的发生率均明显低于汇总的口服研究。在帕利哌酮-LAI 的第 1 周(除运动障碍外的所有 EPS 症状)和口服帕利哌酮治疗时(除帕金森病和震颤外),观察到的发生率最高。与口服研究(17%,P=0.0035)相比,LAI 组(12%)使用抗 EPS 药物的比例显著降低。在研究终点,EPS 量表评分的均值在 LAI 和口服治疗之间相似,且未显示出剂量反应。与基线相比,在研究终点,EPS 量表评分的平均降幅(标准差)在 LAI 组中更大(AIMS:-0.10[1.27];BARS:-0.09[1.06];SAS:-0.04[0.20]),而在口服研究组中更小(AIMS:-0.08[1.32];BARS:-0.03[1.24];SAS:0.0[0.23])。这些变化表明,在研究终点,与 BARS(P=0.023)和 SAS(P<0.0001)相比,LAI 更有利于 BARS 和 SAS,但对 AIMS(P=0.49)则无影响。
在这项事后描述性分析中,与接受约 90 天 LAI 和约 40 天口服帕利哌酮治疗相比,在可比剂量下,自发报告的与 EPS 相关的 TEAEs 的发生率在数值上更低。