Department of Psychiatry and Psychotherapy, School of Medicine, Technical University of Munich, Munich, Germany.
Department of Neuropsychiatry, Keio University School of Medicine, Tokyo, Japan.
Mol Psychiatry. 2023 Aug;28(8):3267-3277. doi: 10.1038/s41380-023-02203-y. Epub 2023 Aug 3.
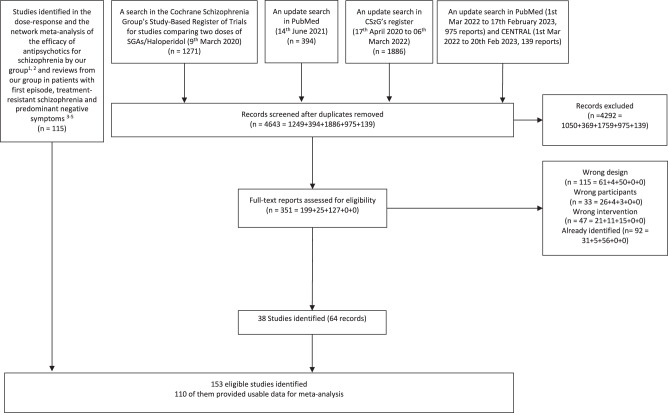
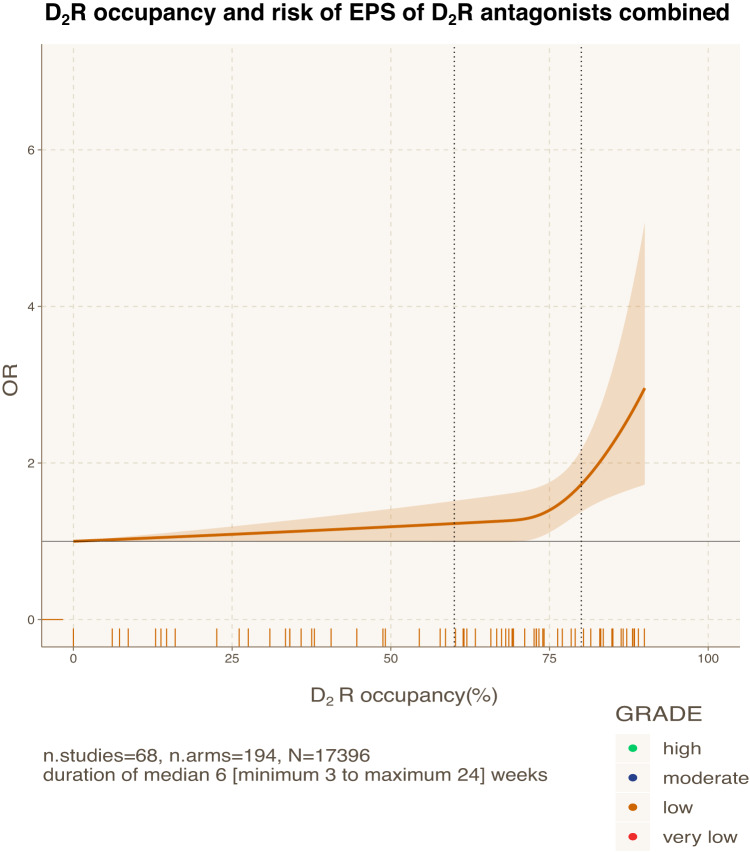
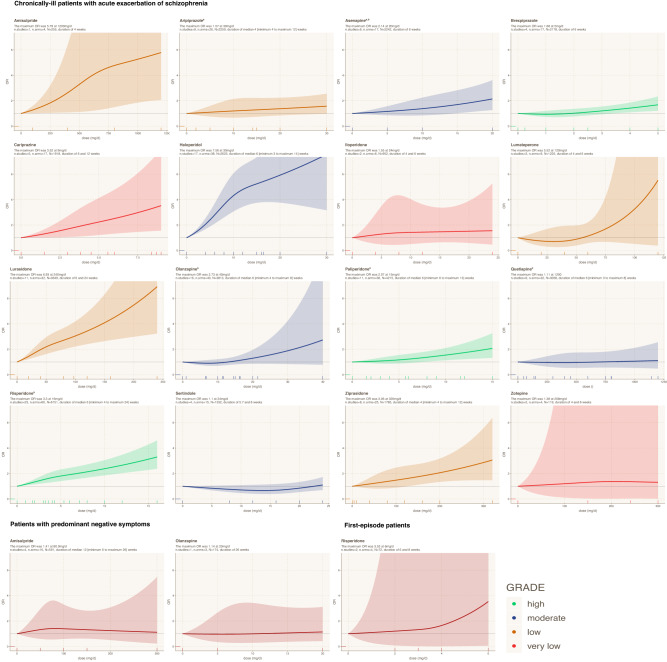
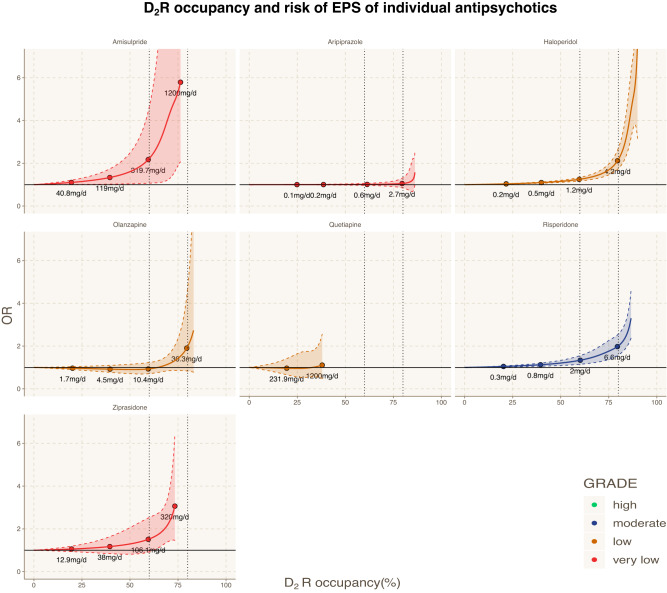
Antipsychotic drugs differ in their propensity to cause extrapyramidal side-effects (EPS), but their dose-effects are unclear. Therefore, we conducted a systematic review and dose-response meta-analysis. We searched multiple electronic databases up to 20.02.2023 for fixed-dose studies investigating 16 second-generation antipsychotics and haloperidol (all formulations and administration routes) in adults with acute exacerbations of schizophrenia. The primary outcome was the number of participants receiving antiparkinsonian medication, and if not available, the number of participants with extrapyramidal side-effects (EPS) and the mean scores of EPS rating scales were used as proxies. The effect-size was odds ratio (ORs) compared with placebo. One-stage random-effects dose-response meta-analyses with restricted cubic splines were conducted to estimate the dose-response curves. We also examined the relationship between dopamine D receptor (DR) occupancy and ORs by estimating occupancies from administrated doses. We included data from 110 studies with 382 dose arms (37193 participants). Most studies were short-term with median duration of 6 weeks (range 3-26 weeks). Almost all antipsychotics were associated with dose-dependent EPS with varied degrees and the maximum ORs ranged from OR = 1.57 95%CI [0.97, 2.56] for aripiprazole to OR = 7.56 95%CI [3.16, 18.08] for haloperidol at 30 mg/d. Exceptions were quetiapine and sertindole with negligible risks across all doses. There was very low quality of findings for cariprazine, iloperidone, and zotepine, and no data for clozapine. The DR occupancy curves showed that the risk increased substantially when DR occupancy exceeded 75-85%, except for DR partial agonists that had smaller ORs albeit high DR occupancies. In conclusion, we found that the risk of EPS increases with rising doses and differs substantially in magnitude among antipsychotics, yet exceptions were quetiapine and sertindole with negligible risks. Our data provided additional insights into the current DR therapeutic window for EPS.
抗精神病药物在引起锥体外系副作用 (EPS) 的倾向方面存在差异,但它们的剂量效应尚不清楚。因此,我们进行了系统评价和剂量-反应荟萃分析。我们检索了多个电子数据库,截至 2023 年 2 月 20 日,以寻找评估 16 种第二代抗精神病药物和氟哌啶醇(所有制剂和给药途径)在急性精神分裂症恶化的成年人中的固定剂量研究。主要结局是接受抗帕金森病药物治疗的参与者人数,如果没有可用的数据,则使用出现锥体外系副作用 (EPS) 的参与者人数和 EPS 评分量表的平均评分作为替代指标。效应大小为与安慰剂相比的优势比 (ORs)。采用受限立方样条进行一阶随机效应剂量-反应荟萃分析,以估计剂量-反应曲线。我们还通过从给药剂量估计占用率来检查多巴胺 D 受体 (DR) 占用率与 ORs 之间的关系。我们纳入了 110 项研究的数据,其中包括 382 个剂量臂(37193 名参与者)。大多数研究是短期的,中位持续时间为 6 周(范围 3-26 周)。几乎所有的抗精神病药物都与剂量相关的 EPS 相关,程度不同,最大的 OR 范围从阿立哌唑的 OR=1.57[0.97,2.56]到氟哌啶醇的 OR=7.56[3.16,18.08],剂量为 30mg/d。喹硫平和曲唑酮是例外,在所有剂量下风险可忽略不计。卡利培嗪、依洛匹隆和佐替平的研究结果质量非常低,氯氮平没有数据。DR 占有率曲线表明,当 DR 占有率超过 75-85%时,风险会显著增加,除了 DR 部分激动剂,尽管 DR 占有率较高,但 OR 较小。总之,我们发现 EPS 的风险随着剂量的增加而增加,并且在抗精神病药物之间的差异很大,但喹硫平和曲唑酮的风险可以忽略不计。我们的数据为 EPS 的当前 DR 治疗窗提供了更多的见解。