Department of Pharmacy, Center for Cell and Gene therapy, The Methodist Hospital, Houston, TX, USA.
Center for Cell and Gene therapy, Baylor College of Medicine, The Methodist Hospital, Houston, TX, USA.
Bone Marrow Transplant. 2014 Feb;49(2):219-22. doi: 10.1038/bmt.2013.149. Epub 2013 Oct 7.
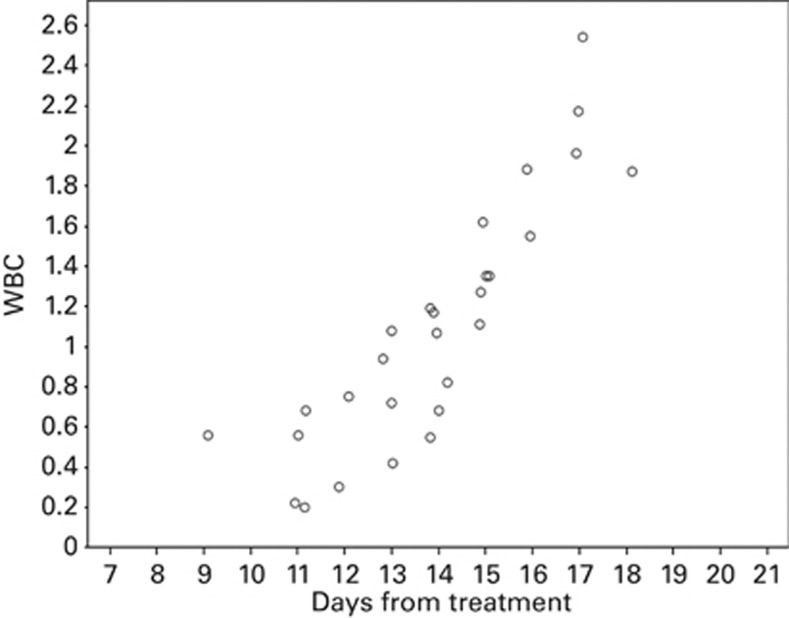
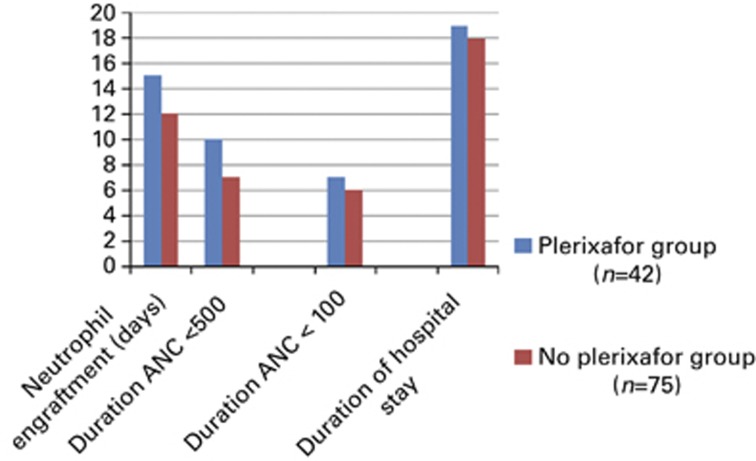
Routine administration of G-CSF following autologous hematopoietic SCT (ASCT) expedites ANC recovery and reduces hospitalization by 1-2 days; it has no impact on febrile neutropenia, infections, morbidity, mortality, event-free survival or OS. To determine whether delayed G-CSF dosage could result in equivalent ANC recovery and thereby improve cost effectiveness, we deferred the administration of G-CSF until WBC recovery had begun. A total of 117 patients with multiple myeloma received ASCT from January 2005 to September 2012. Of these, 52 were in the conventional dosing group (CGD) and received G-CSF from Day +7 for a median of five doses. In the deferred dosing group (DGD), 65 patients received G-CSF from median day 14 post transplant for a median of zero doses. There was no difference between groups in the incidence or duration of febrile neutropenia, duration of grade III mucositis, weight gain, rash, engraftment syndrome or early death (100 days). The DGD group had a significantly longer time to neutrophil engraftment than the CGD group (15 days vs 12 days; P<0.0001), a longer period of severe neutropenia (<100/μL; 8 days vs 6 days; P<0.0001), longer treatment with intravenous antibiotics (7 days vs 5 days; P=0.016) and longer hospital stay (19 days vs 17 days; P=<0.0001). Although the cost of G-CSF was lower in the DGD group (mean $308 vs $2467), the additional hospitalization raised the median total cost of ASCT in this group by 17%. There was, however, no adverse effect of deferred dosing on the rate of febrile neuropenic episodes or Day 100 survival, so that deferred dosing of G-CSF may be suitable for patients receiving ASCT as outpatients, for whom longer hospital stay would not be an offsetting cost.
常规在自体造血干细胞移植(ASCT)后给予 G-CSF 可加速 ANC 恢复并将住院时间缩短 1-2 天;它对发热性中性粒细胞减少症、感染、发病率、死亡率、无事件生存或 OS 没有影响。为了确定延迟 G-CSF 剂量是否可以导致等效的 ANC 恢复,从而提高成本效益,我们延迟了 G-CSF 的给药,直到 WBC 恢复开始。2005 年 1 月至 2012 年 9 月,共有 117 例多发性骨髓瘤患者接受 ASCT。其中,52 例在常规剂量组(CGD)中,从第+7 天开始给予 G-CSF,中位数为 5 剂。在延迟剂量组(DGD)中,65 例患者在移植后中位数第 14 天开始接受 G-CSF,中位数为 0 剂。两组发热性中性粒细胞减少症的发生率或持续时间、III 级粘膜炎的持续时间、体重增加、皮疹、植入综合征或早期死亡(100 天)均无差异。DGD 组的中性粒细胞植入时间明显长于 CGD 组(15 天比 12 天;P<0.0001),严重中性粒细胞减少症的时间较长(<100/μL;8 天比 6 天;P<0.0001),静脉用抗生素治疗时间较长(7 天比 5 天;P=0.016),住院时间较长(19 天比 17 天;P<0.0001)。虽然 DGD 组的 G-CSF 成本较低(平均值为 308 美元比 2467 美元),但额外的住院费用使该组 ASCT 的中位数总费用增加了 17%。然而,延迟剂量对发热性中性粒细胞减少症发作率或第 100 天生存率没有不良影响,因此,对于接受 ASCT 的门诊患者,延迟 G-CSF 剂量可能是合适的,因为他们的住院时间不会成为抵消成本。