Lee Tae Rim, Kang Mun Ju, Cha Won Chul, Shin Tae Gun, Sim Min Seob, Jo Ik Joon, Song Keun Jeong, Jeong Yeon Kwon, Cho Jun Hwi
Crit Care. 2013 Oct 31;17(5):R260. doi: 10.1186/cc13090.
Several methods have been proposed to evaluate neurological outcome in out-of-hospital cardiac arrest (OHCA) patients. Blood lactate has been recognized as a reliable prognostic marker for trauma, sepsis, or cardiac arrest. The objective of this study was to examine the association between initial lactate level or lactate clearance and neurologic outcome in OHCA survivors who were treated with therapeutic hypothermia.
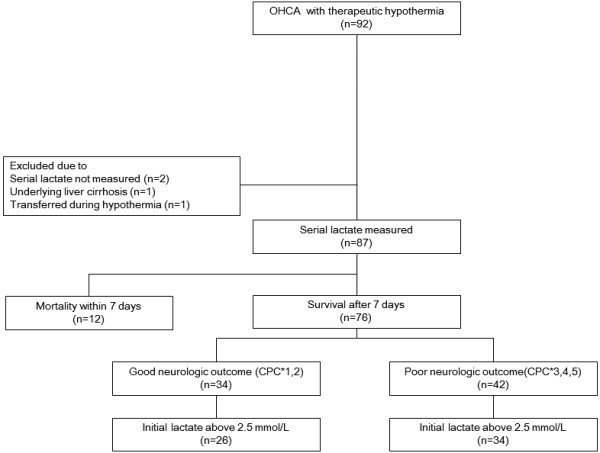
This retrospective cohort study included patients who underwent protocol-based 24-hour therapeutic hypothermia after OHCA between January 2010 and March 2012. Serum lactate levels were measured at the start of therapy (0 hours), and after 6 hours, 12 hours, 24 hours, 48 hours and 72 hours. The 6 hour and 12 hour lactate clearance were calculated afterwards. Patients' neurologic outcome was assessed at one month after cardiac arrest; good neurological outcome was defined as Cerebral Performance Category one or two. The primary outcome was an association between initial lactate level and good neurologic outcome. The secondary outcome was an association between lactate clearance and good neurologic outcome in patients with initial lactate level >2.5 mmol/l.
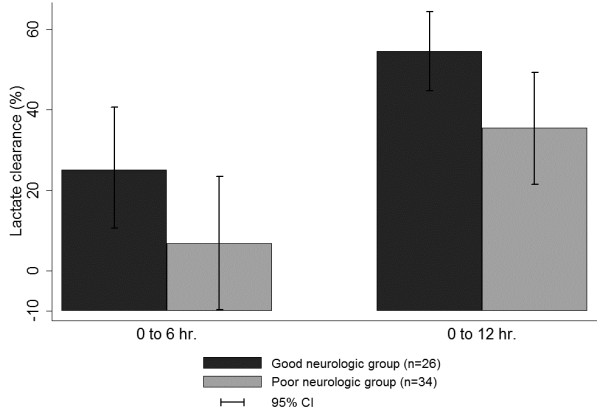
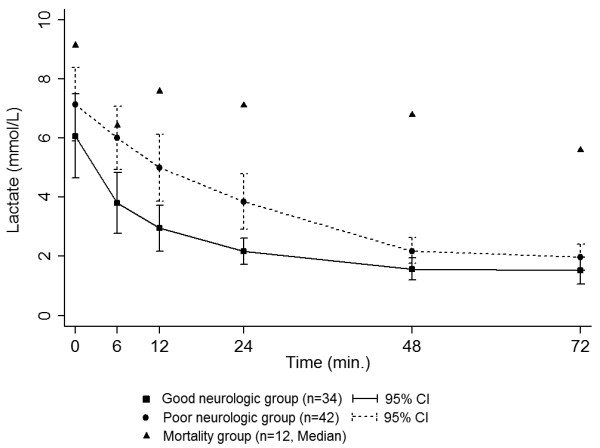
Out of the 76 patients enrolled, 34 (44.7%) had a good neurologic outcome. The initial lactate level showed no significant difference between good and poor neurologic outcome groups (6.07 ±4 .09 mmol/L vs 7.13 ± 3.99 mmol/L, P = 0.42), However, lactate levels at 6 hours, 12 hours, 24 hours, and 48 hours in the good neurologic outcome group were lower than in the poor neurologic outcome group (3.81 ± 2.81 vs 6.00 ± 3.22 P <0.01, 2.95 ± 2.07 vs 5.00 ± 3.49 P <0.01, 2.17 ± 1.24 vs 3.86 ± 3.92 P <0.01, 1.57 ± 1.02 vs 2.21 ± 1.35 P = 0.03, respectively). The secondary analysis showed that the 6-hour and 12-hour lactate clearance was higher for good neurologic outcome patients (35.3 ± 34.6% vs 6.89 ± 47.4% P = 0.01, 54.5 ± 23.7% vs 25.6 ± 43.7% P <0.01, respectively). After adjusting for potential confounding variables, the 12-hour lactate clearance still showed a statistically significant difference (P = 0.02).
The lactate clearance rate, and not the initial lactate level, was associated with neurological outcome in OHCA patients after therapeutic hypothermia.
已经提出了几种方法来评估院外心脏骤停(OHCA)患者的神经功能预后。血乳酸已被公认为是创伤、脓毒症或心脏骤停的可靠预后标志物。本研究的目的是探讨初始乳酸水平或乳酸清除率与接受治疗性低温治疗的OHCA幸存者神经功能预后之间的关联。
这项回顾性队列研究纳入了2010年1月至2012年3月期间在OHCA后接受基于方案的24小时治疗性低温治疗的患者。在治疗开始时(0小时)、6小时、12小时、24小时、48小时和72小时测量血清乳酸水平。之后计算6小时和12小时的乳酸清除率。在心脏骤停后1个月评估患者的神经功能预后;良好的神经功能预后定义为脑功能分类为1级或2级。主要结局是初始乳酸水平与良好神经功能预后之间的关联。次要结局是初始乳酸水平>2.5 mmol/L的患者中乳酸清除率与良好神经功能预后之间的关联。
在纳入的76例患者中,34例(44.7%)具有良好的神经功能预后。良好和不良神经功能预后组之间的初始乳酸水平无显著差异(6.07±4.09 mmol/L对7.13±3.99 mmol/L,P = 0.42),然而,良好神经功能预后组在6小时、12小时、24小时和48小时的乳酸水平低于不良神经功能预后组(3.81±2.81对6.00±3.22,P<0.01;2.95±2.07对5.00±3.49,P<0.01;2.17±1.24对3.86±3.92,P<0.01;1.57±1.02对2.21±1.35,P = 0.03)。二次分析显示,良好神经功能预后患者的6小时和12小时乳酸清除率更高(35.3±34.6%对6.89±47.4%,P = 0.01;54.5±23.7%对25.6±43.7 %,P<0.01)。在调整潜在混杂变量后,12小时乳酸清除率仍显示出统计学显著差异(P = 0.02)。
在接受治疗性低温治疗的OHCA患者中,乳酸清除率而非初始乳酸水平与神经功能预后相关。