Dunlop William, Iqbal Itrat, Khan Ifty, Ouwens Mario, Heron Louise
Mundipharma International Limited, Cambridge, United Kingdom.
Clinicoecon Outcomes Res. 2013 Oct 30;5:555-64. doi: 10.2147/CEOR.S47867. eCollection 2013.
Assessing the cost-effectiveness of treatments in rheumatoid arthritis (RA) is of growing importance due to the chronic nature of the disease, rising treatment costs, and budget-constrained health care systems. This analysis assesses the cost-effectiveness of modified-release (MR) prednisone compared with immediate-release (IR) prednisone for the treatment of morning stiffness due to RA.
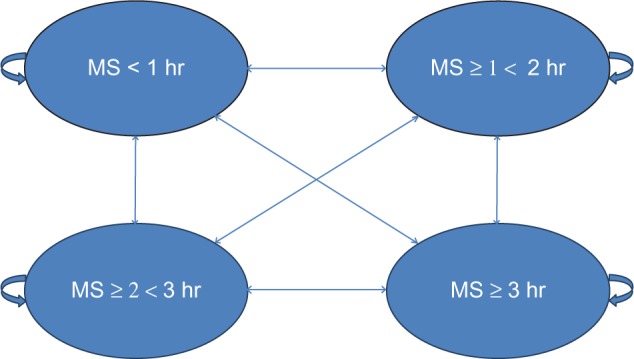
A health state transition model was used to categorize RA patients into four health states, defined by duration of morning stiffness. The model applied a 1-year time horizon and adopted a UK National Health Service (NHS) perspective. Health benefits were measured in quality-adjusted life years (QALYs) and the final output was the incremental cost-effectiveness ratio (ICER). Efficacy data were derived from the CAPRA-1 (Circadian Administration of Prednisone in Rheumatoid Arthritis) study, drug costs from the British National Formulary (BNF), and utility data from a direct elicitation time-trade-off (TTO) study in the general population. Sensitivity analyses were conducted.
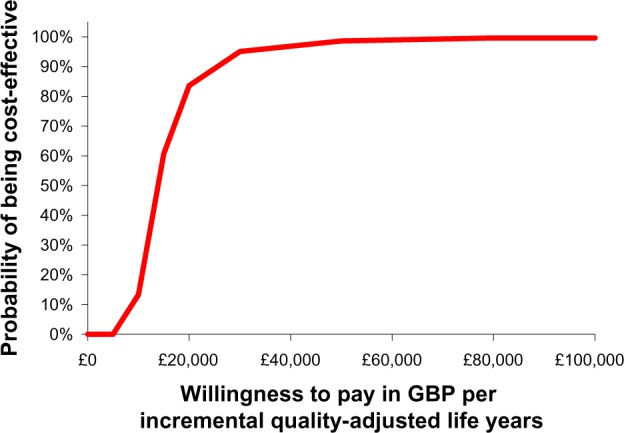
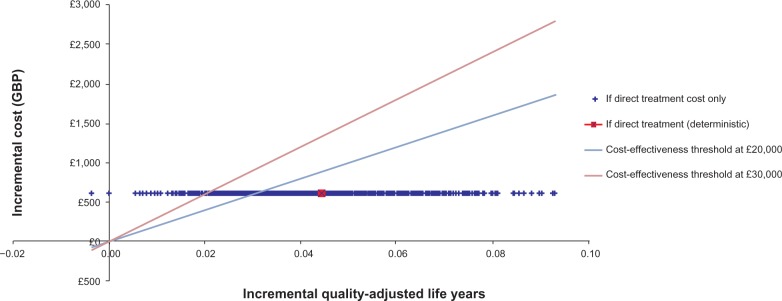
Mean treatment costs per patient were higher for MR-prednisone (£649.70) than for IR-prednisone (£46.54) for the duration of the model. However, the model generated an incremental QALY of 0.044 in favor of MR-prednisone which resulted in an ICER of £13,577. Deterministic sensitivity analyses did not lead to significant changes in the ICER. Probabilistic sensitivity analysis reported that MR-prednisone had an 84% probability of being cost-effective at a willingness-to-pay threshold of £30,000 per QALY. The model only considers drug costs and there was a lack of comparative long-term data for IR-prednisone. Furthermore, utility benefits were not captured in the clinical setting.
This analysis demonstrates that, based on the CAPRA-1 trial and directly elicited public preference values, MR-prednisone is a cost-effective treatment option when compared with IR-prednisone for RA patients with morning stiffness over one year, according to commonly applied UK thresholds (£20,000-£30,000 per QALY). Further research into the costs of morning stiffness in RA is required.
由于类风湿关节炎(RA)的慢性性质、治疗成本不断上升以及医疗保健系统面临预算限制,评估RA治疗的成本效益变得越来越重要。本分析评估了缓释(MR)泼尼松与速释(IR)泼尼松相比治疗RA所致晨僵的成本效益。
使用健康状态转换模型将RA患者分为四种健康状态,根据晨僵持续时间定义。该模型采用1年的时间范围,并采用英国国家医疗服务体系(NHS)的视角。健康效益以质量调整生命年(QALYs)衡量,最终产出为增量成本效益比(ICER)。疗效数据来自CAPRA - 1(类风湿关节炎中泼尼松的昼夜给药)研究,药物成本来自英国国家处方集(BNF),效用数据来自一般人群的直接诱导时间权衡(TTO)研究。进行了敏感性分析。
在模型期间,每位患者的MR - 泼尼松平均治疗成本(649.70英镑)高于IR - 泼尼松(46.54英镑)。然而,该模型得出有利于MR - 泼尼松的增量QALY为0.044,导致ICER为13,577英镑。确定性敏感性分析未导致ICER发生显著变化。概率敏感性分析报告称,在每QALY支付意愿阈值为30,000英镑时,MR - 泼尼松具有84%的成本效益概率。该模型仅考虑药物成本,并且缺乏IR - 泼尼松的比较长期数据。此外,临床环境中未体现效用效益。
本分析表明,根据英国常用阈值(每QALY 20,000 - 30,000英镑),基于CAPRA - 1试验和直接诱导的公众偏好值,对于有一年以上晨僵的RA患者,与IR - 泼尼松相比,MR - 泼尼松是一种具有成本效益的治疗选择。需要对RA中晨僵的成本进行进一步研究。