Department of Epidemiology, Biostatistics, and Occupational Health, McGill University, Montreal, Canada ; Centre for Clinical Epidemiology and Community Studies, Jewish General Hospital, Montreal, Canada.
PLoS One. 2013 Oct 18;8(10):e78548. doi: 10.1371/journal.pone.0078548. eCollection 2013.
Immigrants have increased mortality from hepatocellular carcinoma as compared to the host populations, primarily due to undetected chronic hepatitis B virus (HBV) infection. Despite this, there are no systematic programs in most immigrant-receiving countries to screen for chronic HBV infection and immigrants are not routinely offered HBV vaccination outside of the universal childhood vaccination program.
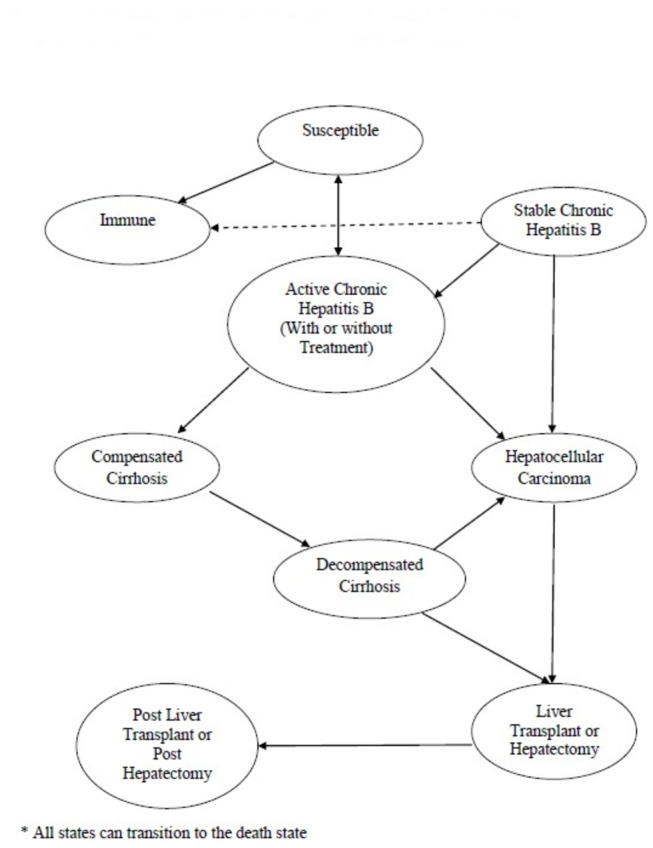
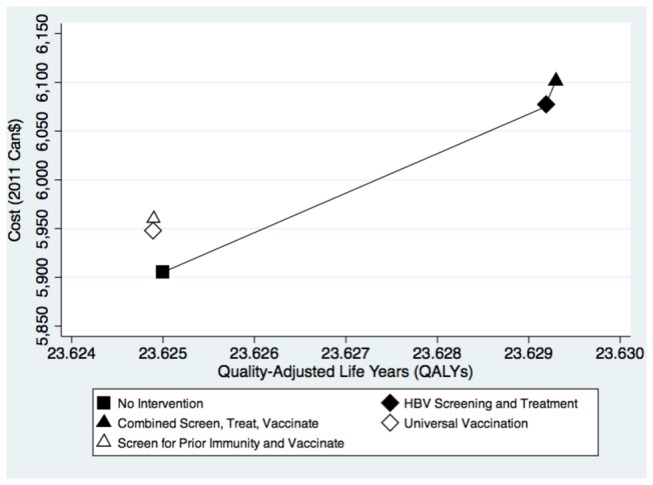
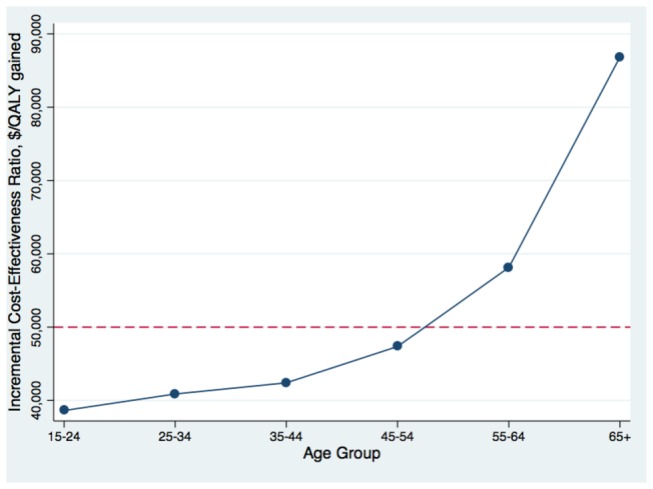
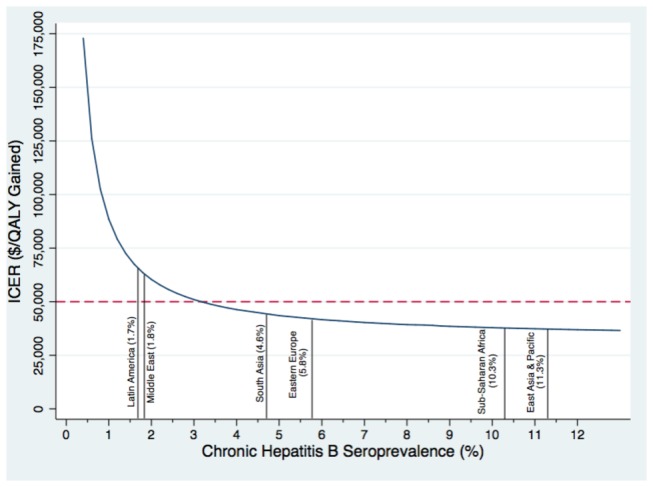
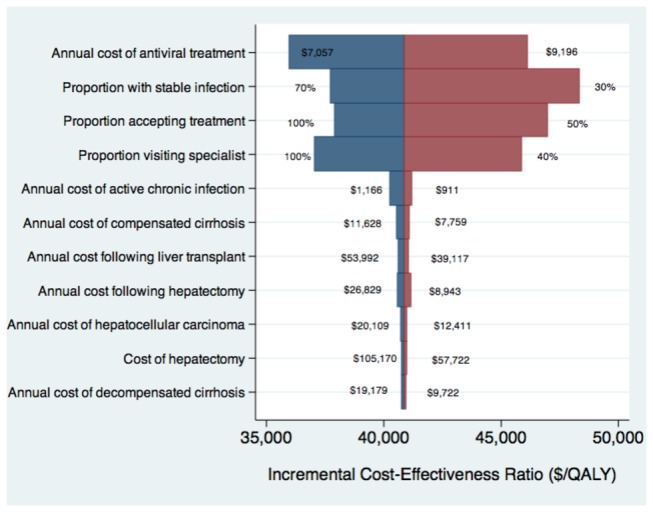
A cost-effective analysis was performed to compare four HBV screening and vaccination strategies with no intervention in a hypothetical cohort of newly-arriving adult Canadian immigrants. The strategies considered were a) universal vaccination, b) screening for prior immunity and vaccination, c) chronic HBV screening and treatment, and d) combined screening for chronic HBV and prior immunity, treatment and vaccination. The analysis was performed from a societal perspective, using a Markov model. Seroprevalence estimates, annual transition probabilities, health-care costs (in Canadian dollars), and utilities were obtained from the published literature. Acute HBV infection, mortality from chronic HBV, quality-adjusted life years (QALYs), and costs were modeled over the lifetime of the cohort of immigrants. Costs and QALYs were discounted at a rate of 3% per year. Screening for chronic HBV infection, and offering treatment if indicated, was found to be the most cost-effective intervention and was estimated to cost $40,880 per additional QALY gained, relative to no intervention. This strategy was most cost-effective for immigrants < 55 years of age and would cost < $50,000 per additional QALY gained for immigrants from areas where HBV seroprevalence is ≥ 3%. Strategies that included HBV vaccination were either prohibitively expensive or dominated by the chronic HBV screening strategy.
Screening for chronic HBV infection from regions where most Canadian immigrants originate, except for Latin America and the Middle East, was found to be reasonably cost-effective and has the potential to reduce HBV-associated morbidity and mortality.
与宿主人群相比,移民的肝细胞癌死亡率更高,主要原因是慢性乙型肝炎病毒(HBV)感染未被发现。尽管如此,在大多数移民接收国中,没有针对慢性 HBV 感染进行筛查的系统计划,并且除了普遍的儿童疫苗接种计划外,通常不为移民提供 HBV 疫苗接种。
对新抵达的加拿大成年移民假设队列进行了一项成本效益分析,以比较四种 HBV 筛查和疫苗接种策略与无干预的情况。所考虑的策略包括:a)普遍接种疫苗;b)筛查既往免疫和接种疫苗;c)慢性 HBV 筛查和治疗;d)慢性 HBV 和既往免疫、治疗和接种疫苗的联合筛查。该分析从社会角度出发,使用马尔可夫模型进行。从已发表的文献中获得了血清流行率估计、年度转移概率、医疗保健成本(加元)和效用。对急性 HBV 感染、慢性 HBV 相关死亡率、质量调整生命年(QALY)和成本进行了建模,涵盖了移民队列的一生。成本和 QALY 按每年 3%的贴现率贴现。筛查慢性 HBV 感染并在有需要时提供治疗被认为是最具成本效益的干预措施,与不干预相比,每获得额外 1 个 QALY 的成本为 40880 加元。对于年龄<55 岁的移民,这种策略最具成本效益,对于来自 HBV 血清流行率≥3%地区的移民,每获得额外 1 个 QALY 的成本将<50000 加元。包括 HBV 疫苗接种的策略要么过于昂贵,要么被慢性 HBV 筛查策略所主导。
对大多数加拿大移民原籍地区(除拉丁美洲和中东地区外)进行慢性 HBV 感染筛查被认为是合理的成本效益措施,有潜力降低 HBV 相关发病率和死亡率。