Department of Otolaryngology, National Taiwan University Hospital, Taipei, Taiwan, R.O.C. ; Department of Otolaryngology, Taipei Hospital, Ministry of Health and Welfare, New Taipei City, Taiwan, R.O.C. ; Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taiwan, R.O.C.
PLoS One. 2013 Oct 25;8(10):e78666. doi: 10.1371/journal.pone.0078666. eCollection 2013.
To investigate the contributions of adenoid and tonsil size to childhood obstructive sleep apnea (OSA) and the interactions between adenotonsillar hypertrophy, age, and obesity in children with OSA.
In total, 495 symptomatic patients were recruited. The patients were assigned to four groups according to age: toddler (age 1-3, n=42), preschool (age 3-6, n=164), school (age 6-12, n=200), and adolescence (age 12-18, n=89). All subjects had tonsil size graded by otolaryngologists, adenoid size determined on lateral radiographs (Fujioka method), and a full-night polysomnography. The apnea-hypopnea index (AHI), adenoid size, and tonsil size were compared in obese and non-obese children in the four age groups. Adjusted odds ratios (ORs) and 95% confidence interval (CI) of adenotonsillar hypertrophy and OSA risk were estimated by multi-logistic regression.
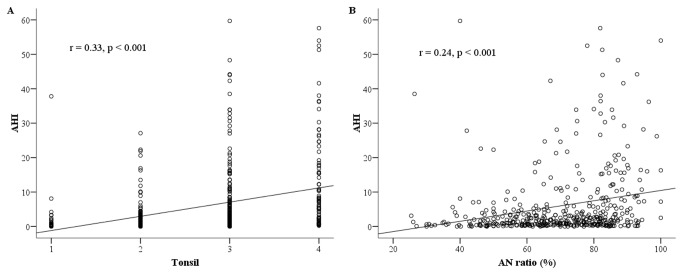
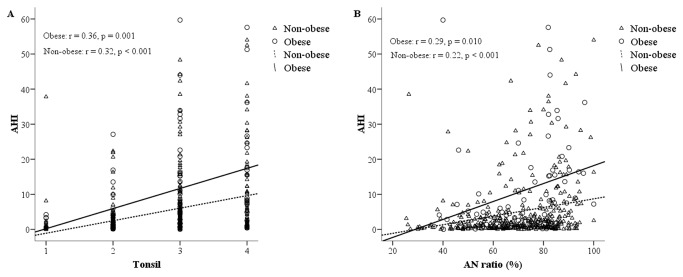
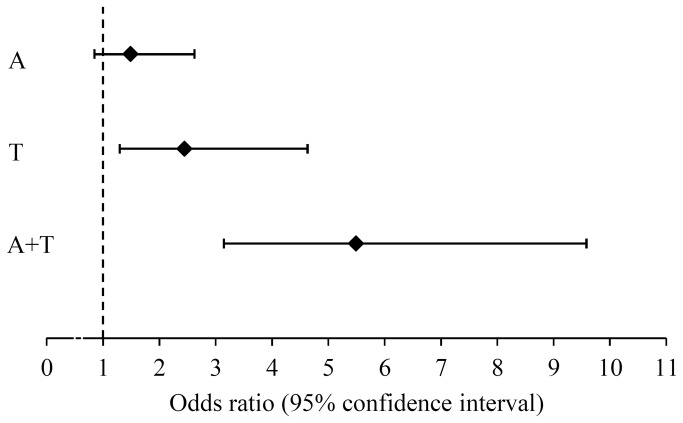
The AHI was positively related to tonsil grade (r=0.33, p <0.001) and adenoid size (r=0.24, p <0.01) in all patients. Tonsil grade was positively related to AHI in all four age groups. Adenoid size was positively related to AHI in the toddler, preschool, school groups, but not in the adolescent group (r=0.11, p=0.37). Tonsil grade and adenoid size were both positively related to AHI in obese and non-obese children. In the regression model, obesity (OR=2.89; 95% CI 1.47-5.68), tonsillar hypertrophy (OR=3.15; 95% CI 2.04-4.88), and adenoidal hypertrophy (OR=1.89; 95% CI 1.19-3.00) significantly increased OSA risk.
Adenotonsillar hypertrophy and obesity are the major determinants of OSA in children. However, the influence of adenoid size decreases in adolescence.
探讨腺样体和扁桃体大小对儿童阻塞性睡眠呼吸暂停(OSA)的影响,以及腺样体扁桃体肥大、年龄和肥胖在儿童 OSA 中的相互作用。
共纳入 495 例有症状的患者。根据年龄将患者分为四组:幼儿组(1-3 岁,n=42)、学龄前组(3-6 岁,n=164)、学龄组(6-12 岁,n=200)和青少年组(12-18 岁,n=89)。所有患者均由耳鼻喉科医生进行扁桃体分级、侧位 X 线片(Fujioka 法)测量腺样体大小,并进行整夜多导睡眠图监测。比较肥胖和非肥胖儿童在四个年龄组中的呼吸暂停低通气指数(AHI)、腺样体大小和扁桃体大小。采用多对数回归估计腺样体扁桃体肥大和 OSA 风险的调整比值比(OR)和 95%置信区间(CI)。
在所有患者中,AHI 与扁桃体分级呈正相关(r=0.33,p<0.001),与腺样体大小呈正相关(r=0.24,p<0.01)。在所有四个年龄组中,扁桃体分级均与 AHI 呈正相关。腺样体大小与 AHI 在幼儿、学龄前和学龄组呈正相关,但在青少年组中无相关性(r=0.11,p=0.37)。在肥胖和非肥胖儿童中,扁桃体分级和腺样体大小均与 AHI 呈正相关。在回归模型中,肥胖(OR=2.89;95%CI 1.47-5.68)、扁桃体肥大(OR=3.15;95%CI 2.04-4.88)和腺样体肥大(OR=1.89;95%CI 1.19-3.00)显著增加 OSA 风险。
腺样体扁桃体肥大和肥胖是儿童 OSA 的主要决定因素。然而,在青少年中,腺样体大小的影响会降低。