Scopelliti Domenico, Fatone Flavia Maria Graziana, Cipriani Orlando, Papi Piero
Department of Cranio-Maxillo-Facial Surgery, Santo Spirito Hospital, Rome, Italy.
Ann Maxillofac Surg. 2013 Jul;3(2):173-7. doi: 10.4103/2231-0746.119229.
So much has been written by so many about secondary procedures in cleft surgery that testify not only the complexity and variable expression of cleft deformity itself but also the need to find methods of primary surgery that will reduce, if not avoid, adverse effects on all the structures and functions involved and affected. It must be the principal aim of cleft surgeon to restore the deformed and displaced regional anatomy to as close to normality as possible, whether or not true hypoplasia exists. The pathogenesis of secondary deformities is related to specific features as: the presence of scar tissues into the cleft basal bone area, that inhibits alveolar growth; scarring of palatal soft tissue, that inhibits growth and causes palatal orientation of dentoalveolar elements; and the exceeding lip tension, that may inhibits maxillary growth along dentoalveolar structures.
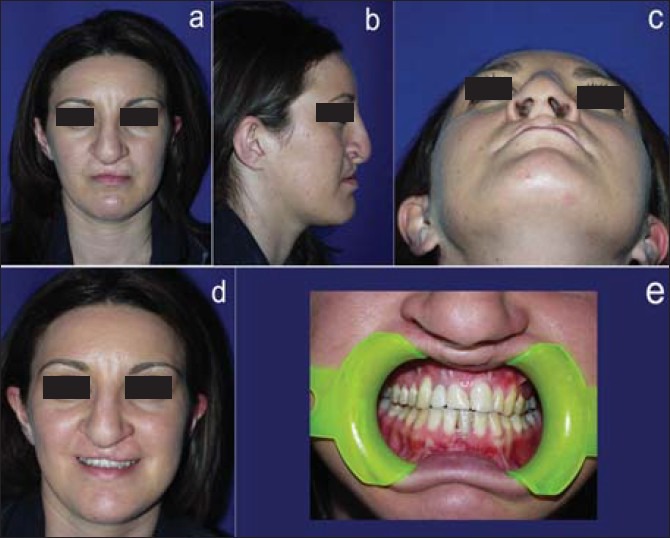
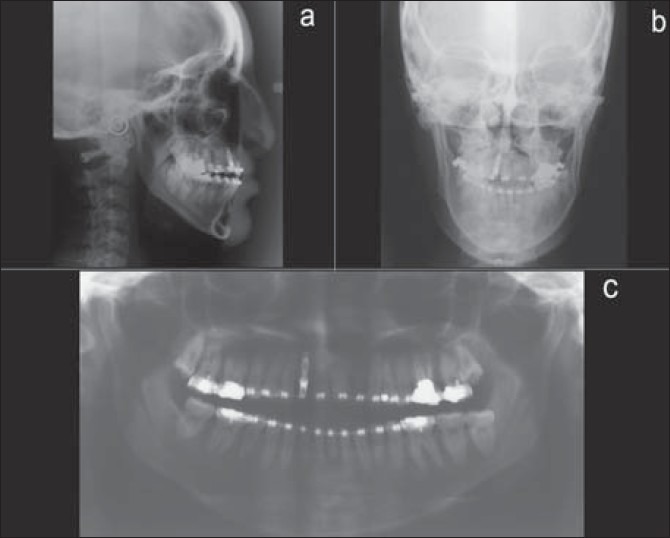
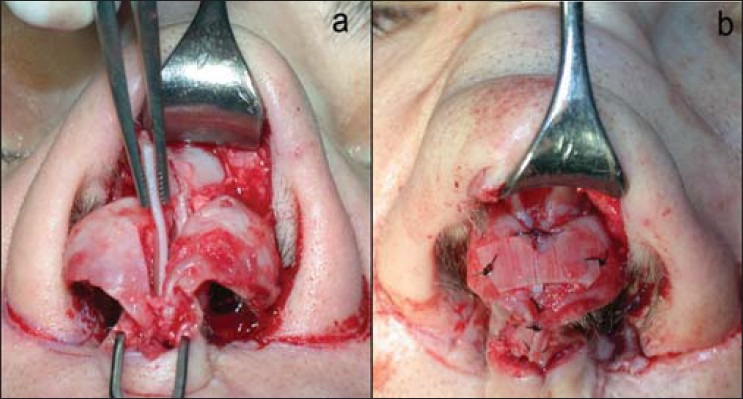
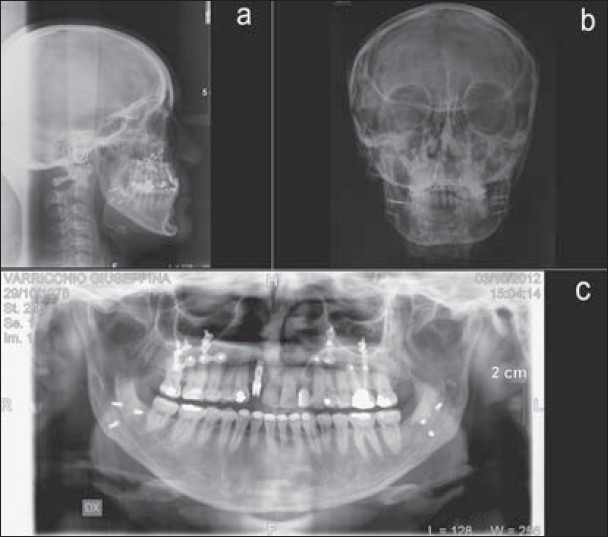
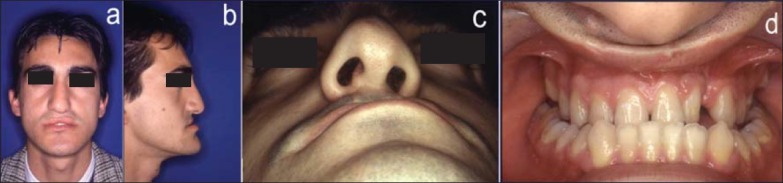
From 2008 to 2011 at the Department of Cranio-Maxillo-Facial Surgery, Santo Spirito Hospital, Rome 25 patients (21 males and 4 females) who had undergone previous surgery for unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP) were enrolled in our study. Diagnosis of deformity was made by means of a cephalometric and photographic analysis (Arnett), gipsometry and a radiological assessment (orthopantomography, lateral and frontal cephalometric X-rays). Moreover, every patient was studied with a temporomandibular joint (TMJ) tomography, TMJ magnetic resonance imaging (MRI) and a computerized gnatography to better evaluate potential TMJ dysfunctions. The surgical procedures adopted simultaneously were: Total or segmental maxillomandibular osteotomies, genioplasty, rhinoplasty, labioplasty, and application of facial prosthesis. Every patient received a postoperative questionnaire to evaluate his/her satisfaction with the surgery performed.
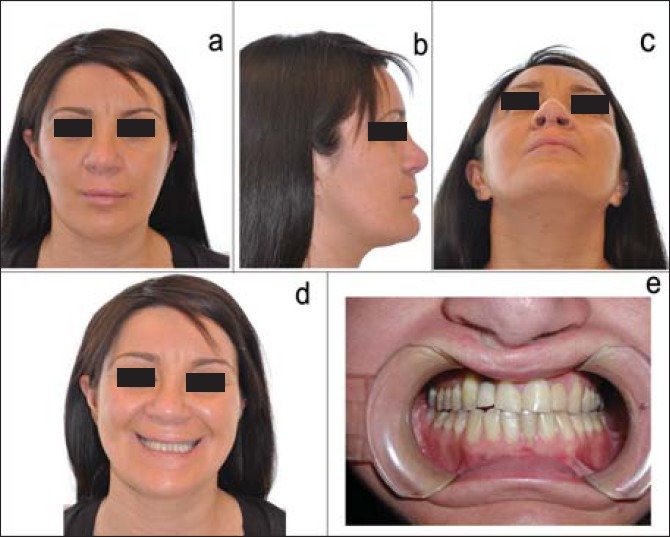
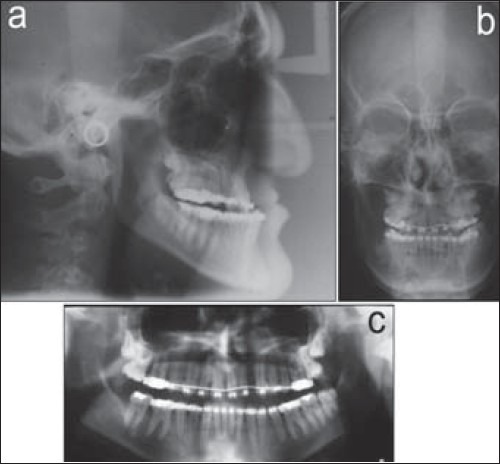
The surgical procedures adopted were Le Fort I osteotomy and bilateral sagittal split osteotomy (BSSO) in 16 patients (65%) and only Le Fort I osteotomy in 9 patients (35%). A relapse of malformation occurred in 4.5% of cases. Concerning the patient questionnaire, 96% of patients were satisfied with the jaw surgery and favorable for combined surgery, 88% were satisfied with lip-nose surgery, and finally 76% would advise to a friend.
Simultaneous correction of the deformities is indicated as to avoid several surgical distresses for the patient, to improve facial aesthetic and function in one surgical step, and to reduce risk of psychological consequences.
关于唇腭裂二期手术,已有众多作者撰写了大量相关内容,这不仅证明了唇腭裂畸形本身的复杂性和多样表现,也表明需要找到一期手术方法,以减少(即便无法避免)对所有涉及和受影响的结构与功能产生的不利影响。唇腭裂外科医生的主要目标必须是将变形和移位的局部解剖结构尽可能恢复至接近正常状态,无论是否存在真正的发育不全。二期畸形的发病机制与以下特定特征相关:腭裂基骨区域存在瘢痕组织,这会抑制牙槽骨生长;腭部软组织瘢痕形成,这会抑制生长并导致牙槽骨结构的腭向移位;以及唇部张力过大,这可能会抑制上颌沿牙槽骨结构的生长。
2008年至2011年期间,罗马圣灵医院颅颌面外科对25例曾接受过单侧唇腭裂(UCLP)和双侧唇腭裂(BCLP)一期手术的患者(21例男性和4例女性)进行了研究。通过头影测量和摄影分析(阿内特法)、石膏模型测量以及放射学评估(曲面断层摄影、侧位和正位头影测量X线片)对畸形进行诊断。此外,对每位患者进行颞下颌关节(TMJ)断层扫描、TMJ磁共振成像(MRI)和计算机化颌面部摄影,以更好地评估潜在的TMJ功能障碍。同时采用的手术方法包括:全上颌或节段性上颌下颌骨截骨术、颏成形术、鼻成形术、唇成形术以及面部假体植入。每位患者术后均收到一份问卷,以评估其对所施行手术的满意度。
16例患者(65%)采用了勒福Ⅰ型截骨术和双侧矢状劈开截骨术(BSSO),9例患者(35%)仅采用了勒福Ⅰ型截骨术。4.5%的病例出现了畸形复发。关于患者问卷,96%的患者对颌骨手术满意并赞成联合手术,88%的患者对唇鼻手术满意,最后76%的患者会向朋友推荐。
一期同时矫正畸形可避免患者承受多次手术痛苦,在一个手术步骤中改善面部美观和功能,并降低心理问题出现的风险。