Department of Cardiology, Fujita Health University, Toyoake, Japan.
BMJ Open. 2013 Nov 11;3(11):e003474. doi: 10.1136/bmjopen-2013-003474.
To study the usefulness of combined risk stratification of coronary CT angiography (CTA) and myocardial perfusion imaging (MPI) in patients with previous coronary-artery-bypass grafting (CABG).
A retrospective, observational, single centre study.
204 patients (84.3% men, mean age 68.7±7.6) undergoing CTA and MPI.
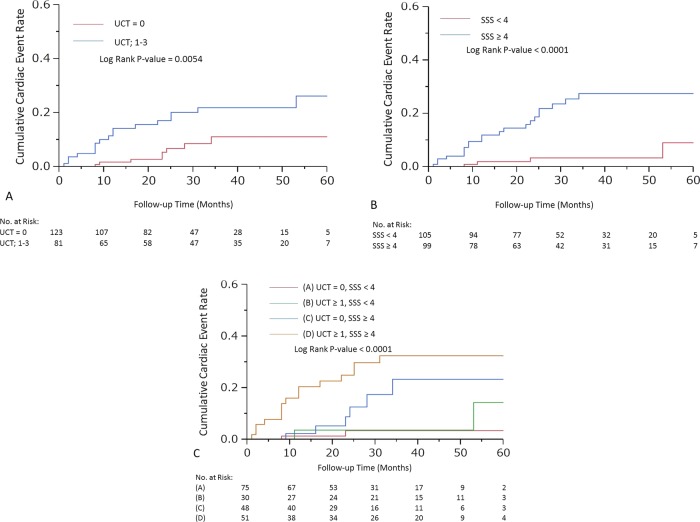
CTA defined unprotected coronary territories (UCT; 0, 1, 2 or 3) by evaluating the number of significant stenoses which were defined as the left main trunk ≥50% diameter stenosis, other native vessel stenosis ≥70% or graft stenosis ≥70%. Using a cut-off value with receiver-operating characteristics analysis, all patients were divided into four groups: group A (UCT=0, summed stress score (SSS)<4), group B (UCT≥1, SSS<4), group C (UCT=0, SSS≥4) and group D (UCT≥1, SSS≥4).
Cardiac events, as a composite end point including cardiac death, non-fatal myocardial infarction, unstable angina requiring revascularisation and heart-failure hospitalisation, were observed in 27 patients for a median follow-up of 27.5 months. The annual event rates were 1.1%, 2%, 5.7% and 12.9% of patients in groups A, B, C and D, respectively (log rank p value <0.0001). Adding UCT or SSS to a model with significant clinical factors including left ventricular ejection fraction, time since CABG and Euro SCORE II improved the prediction of events, while adding UCT and SSS to the model improved it greatly with increasing C-index, net reclassification improvement and integrated discrimination improvement.
The combination of anatomical and functional evaluations non-invasively enhances the predictive accuracy of cardiac events in patients with CABG.
研究经皮冠状动脉血管造影术(CTA)和心肌灌注成像(MPI)联合风险分层在冠状动脉旁路移植术(CABG)后的患者中的应用价值。
回顾性、观察性、单中心研究。
204 例患者(84.3%为男性,平均年龄 68.7±7.6 岁)行 CTA 和 MPI 检查。
通过评估左主干≥50%直径狭窄、其他原生血管狭窄≥70%或旁路血管狭窄≥70%的显著狭窄数量,CTA 定义了未受保护的冠状动脉区域(UCT;0、1、2 或 3 个)。使用接受者操作特征分析的截断值,将所有患者分为 4 组:A 组(UCT=0,总应激评分(SSS)<4)、B 组(UCT≥1,SSS<4)、C 组(UCT=0,SSS≥4)和 D 组(UCT≥1,SSS≥4)。
在中位随访 27.5 个月时,27 例患者发生了心脏事件,作为包括心源性死亡、非致死性心肌梗死、需要血运重建的不稳定型心绞痛和心力衰竭住院的复合终点。A、B、C 和 D 组患者的年事件发生率分别为 1.1%、2%、5.7%和 12.9%(对数秩检验,p<0.0001)。将 UCT 或 SSS 与包括左心室射血分数、CABG 后时间和欧洲危重病评分 II 等有意义的临床因素的模型相结合,可以改善事件预测,而将 UCT 和 SSS 添加到模型中可以显著提高 C 指数、净重新分类改善和综合鉴别改善。
在 CABG 患者中,解剖学和功能评估的联合可提高心脏事件的预测准确性。